
Does Your Child Need a Tonsillectomy?
As a parent, few things are as physically and emotionally draining as watching your child suffer through endless cycles of illness. If you feel like your local Klinik Kesihatan or GP is on speed dial, and your fridge always has a half-empty bottle of pink antibiotics because of your child’s recurrent sore throats, fevers, and sleepless nights—you are certainly not alone.
In Malaysia, our humid tropical climate, occasional haze, and the close-knit, highly social environments of taska(daycare) and tadika (kindergarten) mean that young children are constantly swapping germs. Because of this, tonsillitis feels almost like an unavoidable rite of passage for many kids. But when does it cross the line from a standard, annoying childhood bug to a serious medical issue that requires an ear, nose, and throat (ENT) specialist to intervene?
In decades past, tonsillectomies—the surgical removal of the tonsils—were treated almost as a routine childhood milestone. If a child had a few sore throats, the tonsils were quickly removed. Today, medical professionals take a much more tailored, conservative, and evidence-based approach. The decision to surgically remove a child’s tonsils is not made lightly; it requires carefully weighing the frequency and severity of the child’s infections against the medical risks of surgery.
In this comprehensive guide, we will break down exactly what tonsillitis is, why children are so uniquely prone to it, and the specific medical guidelines that specialists use to determine when a tonsillectomy is truly the best, healthiest course of action for your child.
Understanding the Tonsils: Your Child’s Immune Frontline
Before discussing when to remove them, it is incredibly important to understand what tonsils actually do and why they are there in the first place.
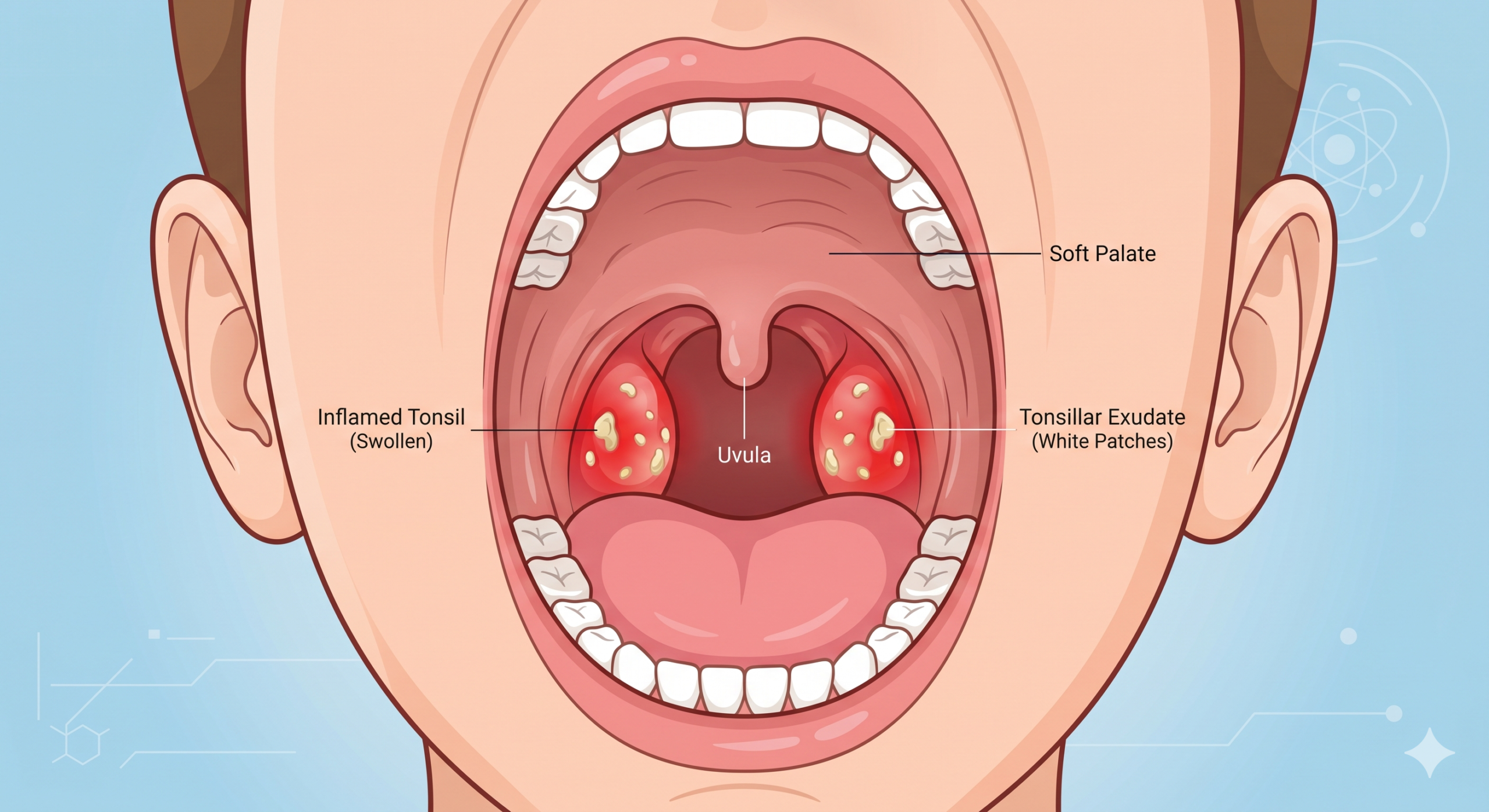
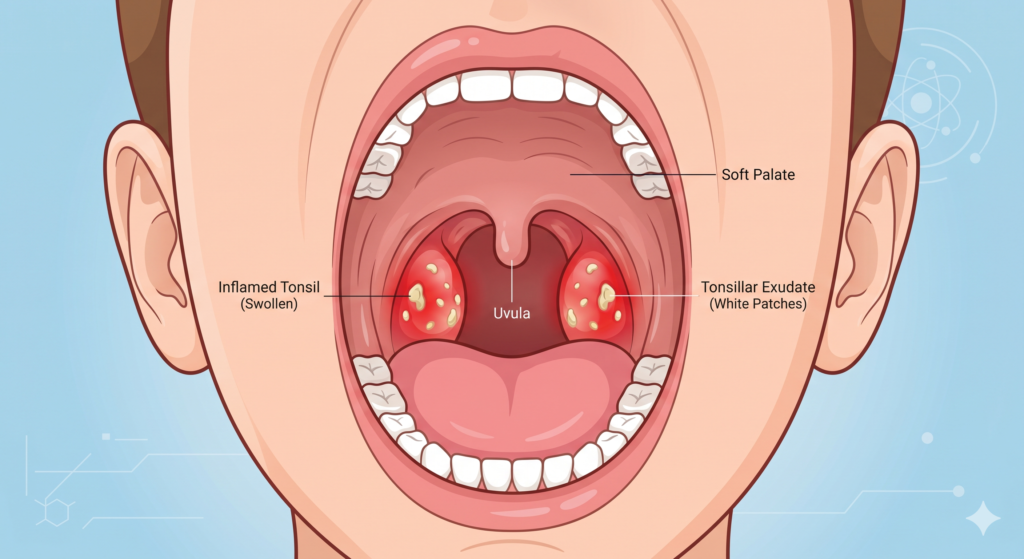
The tonsils are two oval-shaped pads of lymphatic tissue situated at the extreme back of the throat—one on each side. Along with the adenoids (which are located higher up, hidden behind the nasal passages), they form a vital part of the body’s lymphatic system. You can think of them as your child’s biological “first line of defence.”
Because young children are constantly exploring the world—putting shared toys in their mouths, rubbing their faces, and interacting closely with peers—they are exposed to a massive barrage of pathogens daily. The tonsils act like a biological catcher’s mitt. They literally capture viruses and bacteria that enter the body through the mouth and nose, and they produce specialized white blood cells and antibodies to help fight off these invading infections.
However, sometimes this catcher’s mitt becomes completely overwhelmed. When the tonsils themselves become infected and severely inflamed by the very germs they were trying to catch, the result is tonsillitis.
Interestingly, the tonsils are most active in the immune system between the ages of three and seven. As a child grows and approaches puberty, the tonsils naturally shrink and become far less vital to the body’s overall immune defence. The adult immune system is far more robust. This is why teenagers and adults suffer from tonsillitis far less frequently than young, school-aged kids.
What is Tonsillitis? Recognising the Symptoms
Tonsillitis is simply the medical term for an inflammation of the tonsils. It can be triggered by either viral or bacterial infections. Understanding the root cause is crucial because it dictates the entire treatment plan. You can read more in-depth about the specific causes and symptoms of tonsillitis here.
Viral Tonsillitis: The vast majority of tonsillitis cases in Malaysia (up to 70%) are caused by common viruses, such as the rhinovirus (common cold), influenza, or the Epstein-Barr virus. Because it is viral, it must run its course. Antibiotics will be completely ineffective against a virus, and prescribing them unnecessarily only contributes to antibiotic resistance.
Bacterial Tonsillitis: This is most commonly caused by Group A Streptococcus bacteria, universally known as “strep throat.” Unlike viral infections, a confirmed bacterial tonsillitis infection absolutely requires a course of antibiotics to clear the infection and prevent rare but serious complications, such as rheumatic fever or kidney inflammation.
Whether viral or bacterial, the physical symptoms of tonsillitis in children are generally similar and can include:
- Visibly red, painfully swollen tonsils at the back of the throat.
- White or yellow patches (known as exudate) coating the tonsils.
- A severe sore throat that makes swallowing saliva, food, or water difficult or intensely painful.
- A high fever (often exceeding 38.3°C) accompanied by chills and body aches.
- Enlarged, tender lymph nodes (glands) under the jaw or extending down the neck.
- A scratchy, muffled, or throaty “hot potato” voice (as if they have something hot stuck in the back of their throat).
- Noticeably bad breath (halitosis).
- Stomachaches, nausea, or vomiting (particularly common in much younger children and toddlers).
Standard Treatments: The Typical Clinic Visit
When your child is diagnosed with tonsillitis, the immediate medical goal is to keep them as comfortable and well-hydrated as possible while their body’s immune system fights off the infection.
For a viral infection, the best medicine is rest, ample fluids, and over-the-counter pain relievers like paracetamol or ibuprofen to manage the fever and intense throat pain. Warm liquids, like clear chicken broth or warm water with honey (strictly for children over the age of one), and cold treats like popsicles can naturally numb and soothe an inflamed throat.
If the doctor swabs your child’s throat and confirms a bacterial infection, they will prescribe a full course of antibiotics. It is absolutely vital that your child finishes the entire prescription, even if they start feeling back to normal and full of energy after just two or three days. Stopping antibiotics early can lead to the strongest bacteria surviving, mutating, and returning in a stronger, antibiotic-resistant form that is much harder to treat next time.
But what happens when these standard treatments are needed month after month? What happens when your child is constantly sick?
The Tipping Point: When is a Tonsillectomy Recommended?

For many years, the criteria for removing a child’s tonsils were quite subjective. Today, the global medical community relies on strict, evidence-based guidelines, such as those outlined by the American Academy of Otolaryngology-Head and Neck Surgery (AAO-HNS).
Consulting a paediatric ENT specialist is crucial when making this life-changing decision. There are two primary medical reasons an ENT might highly recommend a tonsillectomy for your child: recurrent severe throat infections and sleep-disordered breathing.
1. Recurrent Throat Infections (The Paradise Criteria)
If your child catches tonsillitis once or twice a year, surgery is rarely, if ever, recommended. However, if the infections are chronic, severe, and actively disrupting their quality of life—causing them to miss weeks of school, struggle with academic performance, or forcing you to constantly take unpaid emergency leave from work—an ENT will evaluate them using the internationally recognized “Paradise Criteria.”
According to medical experts at the Mayo Clinic, a tonsillectomy may be highly recommended if your child experiences:
- At least 7 episodes of severe throat infection in the past 1 year.
- At least 5 episodes per year for the past 2 consecutive years.
- At least 3 episodes per year for the past 3 consecutive years.
To be counted as a “severe” episode, the sore throat must be documented by a medical professional and accompanied by at least one of the following: a fever above 38.3°C, swollen and tender lymph nodes in the neck, tonsillar exudate (white/yellow pus spots on the tonsils), or a positive swab test for strep throat.
If your child’s medical history meets these numbers, the long-term health benefits of removing the tonsils to stop the exhausting cycle of sickness generally vastly outweigh the minor, temporary risks of the surgery.
2. Sleep-Disordered Breathing and Pediatric Sleep Apnea
In modern paediatric medicine, this is perhaps the single most common reason for tonsillectomies today. Sometimes, a child’s tonsils and adenoids become so persistently, massively enlarged that they physically block the child’s airway while they are sleeping. This dangerous condition is known as Obstructive Sleep Apnea (OSA).
When a child enters deep sleep, their throat muscles naturally relax. If their tonsils are huge (often referred to as “kissing tonsils” because they touch in the middle of the throat), they collapse inward, temporarily cutting off the child’s oxygen supply. Signs that enlarged tonsils are severely affecting your child’s sleep include:
- Loud, heavy, chronic snoring (a young child should never regularly snore like an adult!).
- Gasping, choking, or visible pauses in breathing during sleep, followed by a sudden snort as they catch their breath.
- Highly restless sleep, tossing and turning frequently throughout the night.
- Chronic mouth breathing during the day (often leading to chapped lips and dental issues).
- Bedwetting in older children who were previously fully potty-trained.
- Daytime behavioural issues, intense hyperactivity, poor school performance, or ADHD-like symptoms caused not by a behavioural disorder, but by sheer, relentless exhaustion.
Pediatric sleep apnea is a profoundly serious condition. Prolonged, night-after-night oxygen deprivation can negatively affect a child’s brain development, cardiovascular health, physical growth, and emotional regulation. In these cases, consulting a sleep apnea specialist for a tonsillectomy (often combined with an adenoidectomy) is highly effective. It frequently provides near-immediate, life-changing relief and dramatically improves the child’s daytime behaviour, growth trajectory, and overall quality of life.
The Procedure: What to Expect on Surgery Day
If you and your ENT specialist decide that a tonsillectomy is the right path forward, knowing exactly what to expect can help ease your parental anxiety and help you prepare your child.
A tonsillectomy is typically performed as a day-case surgery under general anaesthesia. This means your child will be completely asleep, monitored by a dedicated anaesthesiologist, and will feel absolutely zero pain or awareness during the procedure. The surgery itself is surprisingly fast, usually taking only 30 to 45 minutes from start to finish.
The surgeon removes the tonsils entirely through the open mouth using specialised tools—such as electrocautery or radiofrequency wands (coblation)—which remove the tissue and meticulously seal the blood vessels simultaneously to minimise bleeding. There are no external cuts on the face or neck, and no visible stitches.
After the surgery, your child will wake up in a dedicated recovery room. Once they are fully awake, able to independently swallow a little water or apple juice, and their pain is adequately managed by the nursing staff, they are usually allowed to go home on the very same afternoon. For a more detailed, step-by-step breakdown, read our guide on what to expect before, during, and after tonsil surgery.
The Road to Recovery: A Day-by-Day Guide with Local Malaysian Diet Tips

While the surgery itself is remarkably quick, the recovery requires immense patience, diligent pain management, and a lot of tender loving care. According to standard ENT guidelines, full recovery takes roughly 10 to 14 days. The healing process is notoriously non-linear, meaning your child might have a relatively good, energetic day immediately followed by a painful, exhausting day.
Days 1 to 3: The Initial Healing The first few days are characterized by a severely sore throat, a mild low-grade fever, and extreme fatigue as the anaesthesia wears off. Your child will likely complain of severe ear pain; do not panic. This is a very common phenomenon called “referred pain,” where the pain travels from the healing throat to the ears through shared nerve pathways in the head and neck.
- The Goal: Hydration. Dehydration significantly increases pain and is the number one reason children are unexpectedly readmitted to the hospital. Encourage small, frequent sips of cool water, packet apple juice, or ice chips.
- Local Diet Tips: Plain vanilla ais krim or ice lollies are fantastic for naturally numbing the throat. Avoid chocolate or heavy dairy if it makes their mucus feel too thick and difficult to swallow.
Days 4 to 8: The Scab Phase (The Toughest Part) Many parents are caught off guard when the pain suddenly peaks around day 5 or 6. This happens as the thick, white or grey scabs that formed over the surgical sites in the throat begin to naturally peel away and expose the raw, highly sensitive healing tissue beneath. (Note: Many parents mistake these white scabs for pus or a new infection, but they are a totally normal, healthy part of healing!) Bad breath is extremely common and quite potent during this phase.
- The Goal: Strict, round-the-clock pain management. Do not wait for your child to complain of pain. Set alarms during the night to give prescribed painkillers exactly on schedule to stay ahead of the pain.
- Local Diet Tips: Transition to soft, lukewarm, easy-to-swallow foods. Bubur ayam (rice porridge—ensure it is blended smoothly without scratchy bits of fried shallots, peanuts, or ginger), tau fu fah (served cold or room temperature, never hot), soft mee suah in clear broth, and mashed potatoes. Strictly avoid anything spicy (pedas), acidic (like orange juice, pineapple, or lime), or sharp (like crackers or chips), as these can painfully irritate the wound and cause bleeding.
Days 9 to 14: Turning the Corner By the middle of the second week, you should notice a dramatic, rapid improvement in your child’s energy levels, mood, and their pain will steadily subside. They can slowly transition back to their normal Malaysian diet, though they should continue to rest and avoid strenuous physical activity, PE classes, swimming, or playground roughhousing for a full two weeks to prevent delayed bleeding as the final healing takes place.
Risks and Considerations
Like any surgical procedure requiring general anaesthesia, a tonsillectomy carries some risks, though complications are relatively rare. The most significant specific risk associated with this procedure is postoperative bleeding.
While minor, light pink spotting in their saliva or a slightly bloody nose is normal when the scabs begin to fall off, bright red blood or spitting out physical blood clots is a medical emergency. If this happens, do not attempt to look deep inside their throat with a flashlight or let them aggressively gargle. Have them sit upright, spit the blood gently into a bowl, and proceed to the nearest Emergency Department immediately (or call 999).
Other less common risks include post-op infection or severe dehydration due to a steadfast refusal to drink through the pain.
Making the Right Choice for Your Family
Deciding whether to proceed with a tonsillectomy is a collaborative, thoughtful process between you, your child, and your trusted healthcare provider. It requires actively balancing the immense disruption and long-term health risks of constant throat infections or sleep apnea against the temporary pain and slight risks of surgery.
If your child is constantly missing out on their childhood due to severe sore throats, or if their sleep is chaotic, noisy, and restless, do not hesitate to advocate for them. Ask your GP or Klinik Kesihatan doctor for a direct referral to an ENT specialist to get a comprehensive, structural evaluation. By understanding the modern medical guidelines and thoroughly preparing for the recovery process, you can make a confident, informed decision for your child’s long-term health, physical development, and daily happiness.
Frequently Asked Questions (FAQs)
Will removing my child’s tonsils weaken their immune system?
No. Extensive, decades-long medical studies have definitively proven that removing the tonsils does not negatively impact a child’s immune system or make them more susceptible to future illnesses. The human body has hundreds of other lymph nodes and robust immune tissues (including the spleen and bone marrow) to easily compensate for the loss of the tonsils.
Can my child still get strep throat after a tonsillectomy?
Yes, but it is exceedingly rare. The tonsils are the primary breeding ground and “hiding spot” for strep infections, so removing them drastically reduces the frequency of the illness. However, strep bacteria can still occasionally infect the surrounding soft tissues in the back of the throat, though the symptoms are usually much milder.
How long should my child stay home from school or kindergarten after the surgery?
Most children in Malaysia are advised by their ENT surgeons to take a full 10 to 14 days off from school or tadika to adequately recover. They should be eating and drinking normally, sleeping well through the night without severe pain, and be completely off prescription pain medication before returning to the classroom environment.
What is the best thing to eat after getting tonsils out?
In the first few days, liquid hydration is far more important than solid food. Stick to cool water, packet juices (non-acidic), popsicles, and plain ice cream. Once they are ready for solids, opt for soft, bland, room-temperature local foods like smooth bubur, cold tau fu fah, or soft-boiled eggs. Strictly avoid acidic juices, spicy curries, and scratchy snacks like crackers.
Is my child too young for a tonsillectomy?
There is no strict, universal age limit for a tonsillectomy. However, ENT surgeons typically prefer to wait until a child is at least 3 years old, unless severe obstructive sleep apnea is dangerously impacting their breathing, physical growth, or cognitive development. Your ENT will carefully assess the unique risks versus benefits based on your child’s specific age, exact weight, and comprehensive medical history.
Discover more from The ENT Doctor
Subscribe to get the latest posts sent to your email.
Comments are closed