

This is one of the most common conversations I have in my clinic. Not during the first follow-up, when everything is still swollen and we’re both managing expectations. Usually it comes three, six, maybe twelve months later. The patient sits down, looks slightly embarrassed, and says something like: “Doctor, I thought the operation fixed it. But lately… it’s coming back.”
Some of them are genuinely confused because they did feel better — for a while. And a few have already been to a sinseh or tried some herbal remedy because they assumed the surgery had failed and Western medicine had nothing left to offer.
I want to address this properly, because the honest answer is more nuanced than “the surgery failed” — and also more nuanced than “everything is fine, don’t worry.” The recurrence of nasal blockage after surgery is real, it’s common, and whether it means something went wrong depends entirely on why your nose was blocked in the first place.
Surgery Fixes Anatomy. It Does Not Fix Your Immune System.
This is the part nobody explains clearly enough before the operation, and I’ll be direct: that’s partly our fault as surgeons.
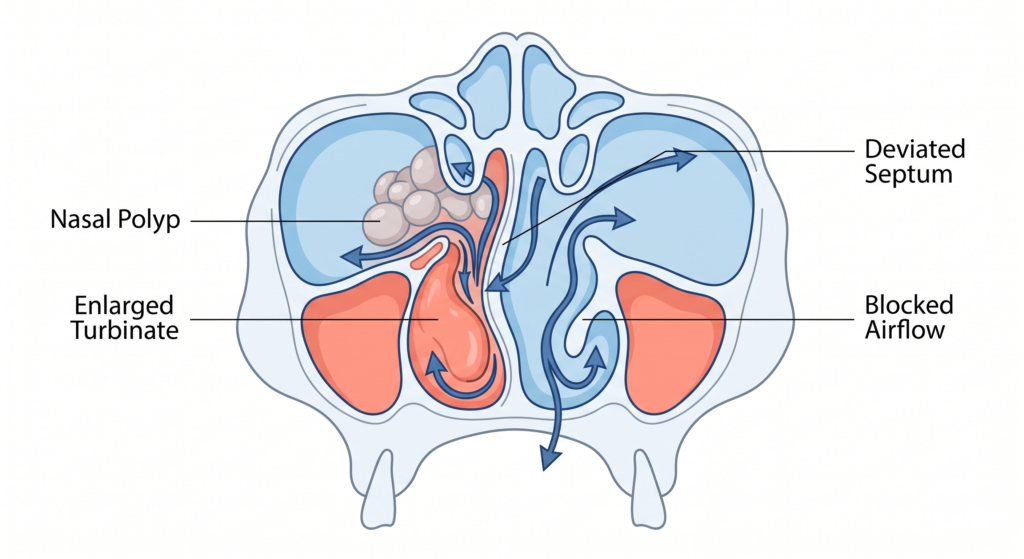
When a patient comes to me with a blocked nose, I’m looking at two broad categories of cause. The first is structural — a deviated septum, enlarged turbinates, nasal polyps, a narrow nasal valve. These are things I can physically correct in an operating theatre. The second is inflammatory — allergic rhinitis, non-allergic rhinitis, chronic rhinosinusitis. These are conditions driven by your immune system, your environment, and in Malaysia specifically, by things like house dust mites, mould spores, haze particles, and pet allergens.
In real patients — the ones sitting in front of me, not the textbook version — both usually coexist.
Your septum is deviated AND you have allergic rhinitis. You have polyps AND underlying chronic sinusitis. Your turbinates are genuinely enlarged AND you’ve been breathing through your mouth for twenty years because of it.
Surgery addresses the first category. It straightens the septum. It reduces the turbinate. It removes the polyps and opens the sinuses. Done well, it creates more space for air to pass through.
But your immune system is still there. Your allergy is still there. The house dust mites in your mattress are still there. The haze season will come back. And when the inflammatory process that was contributing to your blockage starts up again — now in a structurally improved but immunologically unchanged nose — the blockage returns.
This is not a surgical failure. It is a misalignment between what surgery can do and what the patient (and sometimes the surgeon) expected it to do.
The Most Common Reasons Blockage Returns — In Malaysia
Let me go through the specific scenarios I see most often, because they are not all the same problem.
1. Allergic Rhinitis Was Never Controlled

This is by far the most frequent reason. Allergic rhinitis is extremely prevalent in Malaysia — we live in a tropical environment that is essentially paradise for house dust mites, which thrive in heat and humidity. Studies have estimated allergic rhinitis affects somewhere between 30–40% of the Malaysian population, and in my clinical experience that number feels conservative.
A patient with allergic rhinitis has turbinates — the spongy bony structures inside the nose that regulate airflow — that are chronically swollen due to immune activation. Surgery to reduce the turbinate size helps. But if the allergy is not treated alongside the surgery, the turbinates will swell again. Inflammation is relentless. It will use whatever space you gave it.
The correct approach is always surgery plus ongoing medical management. An intranasal steroid spray. Antihistamines when needed. In appropriate patients, allergen immunotherapy. Surgery alone, without addressing the allergy, is like bailing water from a leaking boat without finding the hole.
2. The Septum Shifted (or Was Never the Main Problem)
Septal deviation is one of the most common reasons for septoplasty — the operation to straighten the nasal dividing wall. But cartilage has memory. In younger patients especially, the cartilage can gradually shift back towards its original position over months to years, particularly if the surgery was done before facial skeletal growth had fully completed (generally late teens to early twenties in males).
There is also the sobering reality that not every blocked nose is primarily due to a deviated septum. I see patients who have had septoplasties elsewhere, come to me still blocked, and on examination the septum is actually now fairly straight — but the nasal valve (the narrow triangle at the entrance of the nose) is the real obstruction. Or the inferior turbinates are the main contributors. Fixing the septum without addressing those other components gives incomplete results.
This is why a thorough pre-operative assessment matters. It should involve an endoscopic examination of the nose, sometimes a CT scan of the sinuses, and an honest conversation about what specifically is causing the blockage — and what surgery can and cannot address.
3. Nasal Polyps Grew Back
Nasal polyps are soft, grape-like growths that develop from chronically inflamed sinus mucosa. They are almost always associated with chronic rhinosinusitis — a persistent infection and inflammation of the sinuses. Functional endoscopic sinus surgery (FESS) removes them and opens the blocked sinus drainage pathways.
Polyps recur. This is one of the most frustrating realities of managing chronic rhinosinusitis with polyposis, and I say this as someone who has performed a lot of these surgeries. The recurrence rate varies widely depending on the severity of disease, whether there is associated aspirin sensitivity, and — critically — whether the patient continues with post-operative treatment and follow-up.
The surgery creates better conditions. But the underlying chronic inflammatory process in the mucosa doesn’t disappear. Without regular saline irrigation, intranasal steroids, and surveillance, polyps will grow back. Some patients need revision surgery. A small number with very severe disease may now be candidates for newer biologic therapies — injectable medications that target the specific immune pathways driving polyp formation — though availability and cost in Malaysia is still a significant barrier.
4. Scar Tissue Formed After Surgery
This one is genuinely related to the surgery itself. Any healing wound produces scar tissue — that’s normal biology. Inside the nose, where surfaces are close together and the environment is moist, adhesions can sometimes form between the septum and the turbinate, or between the lateral nasal wall and the middle turbinate. These are called synechiae.
They can partially obstruct airflow even in an otherwise well-executed operation. They usually form in the first few weeks after surgery and may not be noticed by the patient immediately because the surrounding postoperative swelling masks them initially. As the swelling settles, the adhesion becomes the dominant obstruction.
This is why postoperative follow-up is not optional. The first few weeks are critical for identifying and releasing any early synechiae before they mature into firm fibrous scar bands.
5. You Stopped the Nasal Spray Too Early
This one I will say plainly: it happens constantly.
Patients feel better after surgery. The nose is open, they can breathe, they are sleeping better. They stop the intranasal steroid spray because they feel fine and figure the surgery has sorted things out. Three months later, the allergy-driven inflammation that was being suppressed by the spray has quietly rebuilt itself, and the blockage is creeping back.
Intranasal steroid sprays (like fluticasone, mometasone, budesonide) are not a short-term fix. For patients with allergic rhinitis or a history of polyps, they are long-term maintenance — often indefinite. The goal is not to treat symptoms when they occur. The goal is to suppress the chronic inflammatory process that leads to recurrent obstruction.
Stopping the spray because you feel well is a bit like stopping blood pressure medication because your blood pressure is now normal. The medication is why it’s normal.
A Word About Traditional Remedies and Sinusitis
I’m going to mention this because it comes up, not to dismiss anyone’s beliefs.
Many Malaysian patients — use the term resdung to describe their nasal symptoms, and there is a well-established market for traditional treatments: ubat herba, steam inhalation with serai wangior kapur barus, bekam (cupping), and various supplements. Some patients try these before surgery, some try them when symptoms recur after surgery.
I do want to be clear: none of these address the anatomical or immunological processes I’ve described above. They may offer temporary symptomatic relief — steam humidifies the nasal mucosa, warmth may temporarily shrink blood vessels — but they do not correct a deviated septum, remove polyps, or treat allergic sensitisation to house dust mites.
When blockage returns after surgery and a patient reaches for traditional remedies first, months can pass before they come back to the clinic. By that time, polyps may have regrown substantially, or an adhesion that could have been released simply in the clinic has become a firm scar. Early review is always better.
What You Should Realistically Expect From Nasal Surgery

This is the conversation I try to have before every operation, and I’ll put it here for those who are considering surgery or who have had it and are now confused about what happened.
Septoplasty for a deviated septum — this addresses the structural blockage. If allergy is also present and not treated, you may still have partial blockage from turbinate swelling, and you will likely need ongoing medical management. The structural improvement is generally permanent in adults. The functional result depends on whether everything contributing to the blockage has been addressed.
Turbinate reduction — this reduces the volume of the turbinates. The bone component stays reduced. The mucosal component (which swells due to allergy and inflammation) can swell again if the underlying condition is not managed. This is not recurrence of the turbinate enlargement in the structural sense — it is the inflammatory tissue doing what inflammatory tissue does.
FESS for chronic rhinosinusitis and polyps — this clears the polyps and restores drainage. It does not cure chronic rhinosinusitis. Think of it as creating the best possible conditions for the disease to be managed medically. Post-operative care — nasal irrigation, topical steroids, follow-up — is not optional. It is the other half of the treatment.
Surgery, done well, gives you a better baseline. It does not give you a new nose that is immune to what your old nose was dealing with.
When You Should Come Back and See Us
If your nose was operated on and the blockage is returning, please don’t wait. Come back when:
- Blockage returns more than three months after surgery seemed to have resolved it
- You notice a change in sense of smell (this can indicate early polyp regrowth)
- The blockage is one-sided and worsening (this always warrants proper assessment)
- You are no longer getting relief from your nasal spray
- You develop facial pressure, thick discoloured nasal discharge, or recurrent sinusitis
And if you were told after your operation to use a nasal spray and do saline rinses and come back in three months — and you did none of those things — please come back anyway. We are not going to lecture you. But we do need to see what’s happening.
The Bottom Line
Nasal surgery is not a one-time fix for a problem that goes away permanently. For many patients it produces dramatic, lasting improvement. For others — particularly those with significant allergic rhinitis, polyps, or chronic sinusitis — it is the beginning of long-term management, not the end of it.
The question “why is my nose blocked again after surgery?” usually has a specific, answerable reason. Sometimes it’s the allergy that was never fully controlled. Sometimes it’s scar tissue. Sometimes the surgery addressed one problem but not all of them. Occasionally there is a technical consideration worth reviewing.
What it almost never is: a reason to give up on treatment entirely, or to conclude that surgery was pointless.
For further questions, feel free to contact us via this link.
Dr. Julius Goh Liang Chye is a Consultant Otorhinolaryngologist at Universiti Malaya Specialist Center, with expertise in rhinology and nasal surgery . For appointments and consultations, contact us here.
Discover more from The ENT Doctor
Subscribe to get the latest posts sent to your email.
Comments are closed