
When a patient tells their relatives they are seeing an ENT surgeon about their nose, and I mention the word rhinoplasty, the reaction is usually the same. Eyebrows go up. Someone makes a comment about wanting a sharper nose. The patient laughs awkwardly. And then I spend ten minutes explaining that what we are actually discussing has nothing to do with looking like a Korean celebrity.
This happens more than I’d like to admit.
Rhinoplasty — the surgical reshaping of the nose — carries an enormous amount of cultural baggage in Malaysia. The word immediately conjures images of the before-and-after photos you see in aesthetic clinic advertisements, or stories about someone flying to Seoul or Bangkok for a “nose thread lift.” For most Malaysians, rhinoplasty sits squarely in the category of vanity procedures, something you do because you’re unhappy with how you look, not something a hospital surgeon recommends for medical reasons.
That assumption is wrong, and it stops a meaningful number of patients from seeking help that could genuinely change their quality of life.
Two Completely Different Operations That Share a Name
Let me draw the line clearly, because the medical world doesn’t always do this well.
Cosmetic rhinoplasty is what most people picture. It changes the appearance of the nose — reducing a dorsal hump, refining the tip, building up a flat nasal bridge with implants. The patient’s breathing may be perfectly fine. The goal is purely aesthetic. This is what aesthetic clinics and plastic surgeons advertise, and it is elective in the truest sense.
Functional rhinoplasty is a different operation with a different purpose. It corrects structural problems inside and outside the nose that are causing the patient to breathe poorly, sleep badly, or suffer chronic nasal symptoms. The external appearance of the nose may change as a side effect of correcting the underlying problem, but that is not the goal.
And then there is septorhinoplasty — where both are done together. The functional problem is corrected, and at the same time, the external appearance is improved. This is common, entirely legitimate, and in many cases makes practical sense since we are already operating in the same anatomical area.
The confusion between all three — and the blanket assumption that any nose surgery is cosmetic — is what I want to address here.
Why Malaysian Noses, Specifically, Have Functional Problems
I’m going to say something that is clinically accurate and not meant to offend anyone: the typical Southeast Asian nasal structure presents specific functional challenges that East Asian, South Asian, and Caucasian noses do not share to the same degree.
Broadly speaking, Malay, Chinese Malaysian, and to a lesser extent Indian Malaysian patients tend to have wider nasal bases, shorter columellae (the strip of tissue between the nostrils), and weaker lower lateral cartilages compared to Caucasian patients. The nasal tip may lack projection, and the cartilage framework providing structural support to the nasal valve — the narrowest functional point inside the nose — is often less robust.
This matters because the nasal valve, which sits just inside the nostril opening, is responsible for a significant portion of nasal airflow resistance. When the cartilage supporting it is weak or when the valve collapses inward during inhalation, breathing through the nose becomes genuinely difficult — not because of allergy or infection, but because the physical architecture of the airway is insufficient.
Some patients have lived with this their entire lives and simply accepted that they are “not a nose breather.” Others develop increasing symptoms as they age and the cartilage loses even more structural integrity. And a significant number have had prior nasal trauma — a road accident, a sports injury, a childhood fall — that disrupted the already limited structural support and created a functional problem that no amount of nasal spray will correct.
The Most Common Functional Problems we encounter

Nasal Valve Collapse
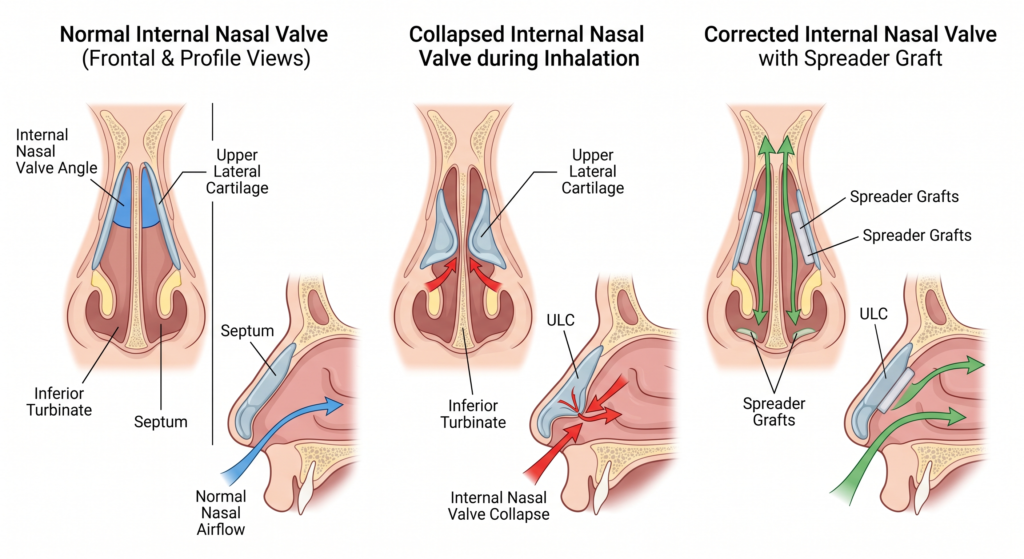
This is the most underdiagnosed cause of nasal obstruction I encounter. The nasal valve — both the internal and external components — can collapse during nasal breathing, particularly during deep inhalation. If you try to breathe in hard through your nose and the sides of your nostrils suck inward, that is external nasal valve collapse. If there is no visible movement but breathing feels like inhaling through a slightly squashed straw, internal valve compromise is likely.
The Cottle manoeuvre — where placing a finger against the cheek and pulling the cheek gently outward suddenly improves nasal breathing — is a simple bedside test I use regularly. If breathing improves dramatically with that gentle lateral traction, nasal valve compromise is contributing to the obstruction.
This is not fixed by medication. It is fixed by surgery that supports and widens the valve using cartilage grafts — specifically, a spreader graft placed between the septum and the upper lateral cartilage, or an alar batten graft supporting the external valve. The technique involves working with cartilage from the septum or ear, restructuring the nasal framework to hold open during breathing. The result changes the shape of the nose slightly. But the goal was function, not aesthetics.
Post-Traumatic Nasal Deformity
Malaysia’s road accident statistics are sobering. Nasal fractures are among the most common facial injuries from motorcycle accidents, and they are frequently undertreated. The acute swelling is managed, perhaps a simple manipulation is done under sedation if the fracture is fresh, and then the patient is discharged with instructions to follow up — which often doesn’t happen.
Years later I see these patients. The nose has healed in a deviated position. The septum is badly displaced, often touching the lateral nasal wall on one side. Breathing through that side is nearly impossible. The external nose is visibly crooked.
This is a functional problem. The operation to correct it — a septorhinoplasty — straightens the septum, removes or repositions the deviated cartilage and bone, and restores symmetry to the external nose. It is not performed because the patient is unhappy with aesthetics. It is performed because they cannot breathe properly after an injury, sometimes for ten or twenty years.
When I explain this to patients who have been told by their GP that “nothing can be done” about their crooked post-accident nose, their reaction is usually a mixture of relief and frustration. Relief that there is an answer. Frustration that nobody had told them sooner.
Saddle Nose Deformity
The dorsum of the nose — the bridge — is supported by both bone above and cartilage below. When the cartilage support is lost, whether from previous nasal surgery that removed too much septum, from untreated septal haematoma after trauma, or from inflammatory conditions like Wegener’s granulomatosis or cocaine use, the bridge collapses inward. The resulting shape gives the nose a flattened or concave profile — the so-called saddle deformity.
This looks cosmetically obvious, but it also causes functional problems. The collapsed bridge narrows the internal nasal space, disrupts airflow, and may be accompanied by a perforated septum. Repair involves reconstructing the structural support with cartilage grafts — rib cartilage is often needed for significant defects — and this is a complex procedure I want patients to understand as reconstructive, not aesthetic.
The Crooked Nose After Septal Surgery
This one is specific and worth mentioning because I see it in the context of prior nasal operations. Occasionally a septoplasty done elsewhere results in a nose that, while internally better, has become slightly crooked or the tip has lost support because too much cartilage was removed. The patient trades one problem for another.
Revision surgery to restore tip support and correct external deviation after a previous septoplasty is absolutely within the category of functional surgery. It is also technically demanding — working in a nose that has already been operated on always introduces scar tissue and altered anatomy that make the surgery more challenging.
What About The Patients Who Want Both?
This is a question I actually appreciate being asked directly, because the answer is honest: yes, some patients who need functional rhinoplasty would also like to improve the appearance of their nose at the same time, and there is nothing wrong with that.
If I am already operating on the septum, the nasal valves, and the cartilage framework to improve breathing, the incremental cost of also refining the tip or improving the profile is relatively small in terms of surgical risk and recovery. The structures are already being accessed. The patient goes to sleep once, recovers once, and addresses both the function and the form in a single procedure.
I am straightforward with patients about this. There is a distinction between the medically indicated portion of the surgery — which should form the basis of any consultation — and the cosmetic component. A government hospital like UMMC operates on a case-by-case basis regarding what can be done in a public setting versus what would require the patient to be referred to a private facility. But in principle, combined functional-cosmetic rhinoplasty is a real option and a reasonable conversation to have.
What I don’t do is lead with aesthetics for a patient presenting with a breathing problem. That is not the right frame for someone who came because they cannot breathe through their nose at night.
The Taboo Conversation: Is Wanting to Look Better a Problem?
I’ve thought about how to write this section carefully, because Malaysia is a multi-ethnic, multi-faith country and attitudes toward elective cosmetic procedures vary widely across communities.
Some patients I see — particularly from more conservative backgrounds — would never present saying they want their nose to look different. It would feel vain. It would invite judgment from family. But when I explain that what we are discussing is a functional operation that will also change the shape somewhat, and I show them what the result might look like, the honest reaction is often: “Actually, doctor, I don’t mind if it looks a bit better too.”
That’s a very human response. There is nothing clinically or ethically wrong with a patient wanting both function and a better appearance from a single operation. The problem arises when cosmetics drives clinical decision-making — when a surgeon recommends structural changes that serve aesthetics but compromise nasal physiology. That is what I want patients to be alert to, regardless of whether they are seeing an ENT or a plastic surgeon.
ENT Surgeon vs. Plastic Surgeon: Who Should Do Your Functional Rhinoplasty?
This question comes up and deserves a direct answer.
Plastic surgeons trained in rhinoplasty have expertise in external nasal anatomy, aesthetic outcomes, and cartilage manipulation. ENT surgeons trained in rhinology have deep expertise in the internal nasal airway, the septum, the turbinates, and the sinus system. A rhinoplasty for purely cosmetic purposes sits comfortably in a plastic surgeon’s skillset. A septorhinoplasty where the primary purpose is to restore nasal airflow — particularly when there are internal structural problems, valve issues, or prior sinus surgery complicating the picture — is a case where ENT expertise in airway anatomy is directly relevant.
In an ideal world, complex cases are managed collaboratively. In Malaysia’s current surgical landscape, the right question to ask any surgeon you are consulting is: “How much of your rhinoplasty practice is functional versus cosmetic?” The answer will tell you a great deal.
What Recovery Looks Like

Patients considering functional rhinoplasty often worry about the social aspect of recovery — the bruising, the swelling, the splint, the explaining to colleagues and relatives what happened. This is a legitimate concern, and I’d rather be upfront about it than dismiss it.
Swelling is most significant in the first two weeks. The external splint, if used, is worn for about a week. Bruising around the eyes is common. Most patients take one to two weeks off work. The nose continues to refine over months — final results are typically visible at six to twelve months, because nasal skin, particularly thicker Southeast Asian skin, takes time to re-drape over the new framework.
Internally, breathing improvement is often noticed as soon as the postoperative swelling settles, usually by week three to four. This is usually the moment patients tell me they understand why the surgery was worth doing.
The Bottom Line
Rhinoplasty is not just a nose job. For a meaningful number of patients — those with nasal valve collapse, post-traumatic deformity, structural breathing obstruction — it is a functional operation that belongs in the same category as a septoplasty or a turbinate reduction. The difference is that it addresses not just the internal septum and turbinates, but the entire structural framework of the nose.
If you have been told nothing can be done about your breathing because your nose looks normal on a CT scan, or because your septum is not severely deviated, ask specifically about nasal valve assessment. If your nose has been crooked since an accident and you have always breathed poorly on one side, that is worth a proper evaluation.
And if you quietly also want to know whether the shape can be improved at the same time — just ask. There is no judgment in that question.
Dr. Julius Goh Liang Chye is a Consultant Otorhinolaryngologist at Universiti Malaya Specialist Center For appointments and consultations, contact us here
Discover more from The ENT Doctor
Subscribe to get the latest posts sent to your email.
Comments are closed