
A question that comes up in my clinic more often than you might expect: “Doctor, if I wait long enough, will my tonsils just shrink on their own?”
Sometimes it comes from a parent holding out hope before their child goes to the operating theatre. Sometimes it is an adult who has had four courses of antibiotics in six months and wants to believe there is a fifth option. And increasingly it is coming from patients who have seen social media posts claiming that certain medications, supplements, or lifestyle changes can cause tonsil tissue to “regress.”
The honest answer is: yes, tonsils can shrink. But the conditions under which that happens are quite specific — and for a meaningful proportion of patients, by the time they are sitting in my consultation room, those conditions no longer apply. Let me explain exactly why.
What Tonsils Are Actually Doing in the First Place
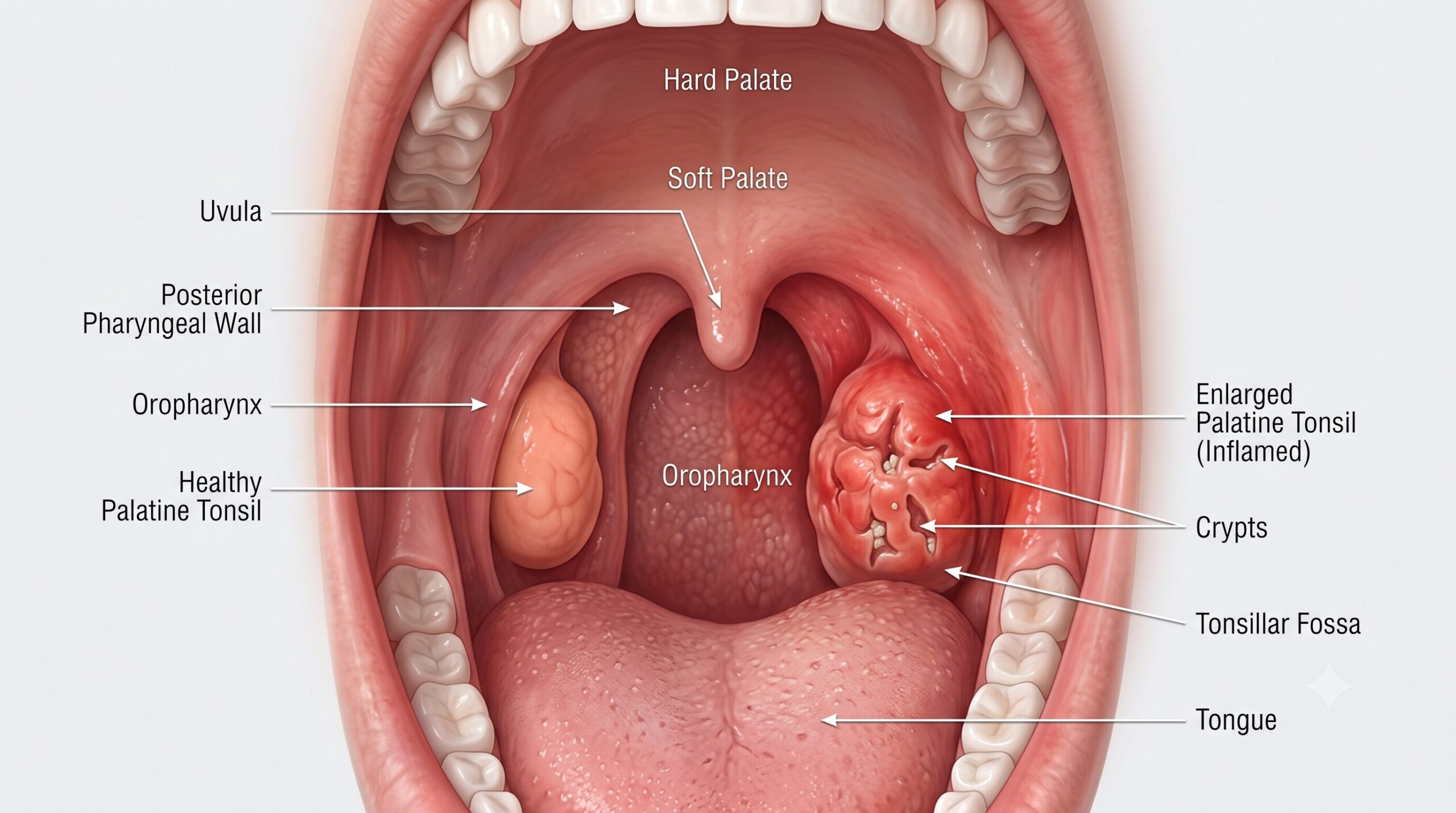
Your palatine tonsils — the two lumps of tissue at the back of your throat that most people mean when they say “tonsils” — are not useless decorations. They are part of Waldeyer’s ring, a band of lymphoid tissue that forms the immune system’s first line of defence against inhaled and ingested pathogens. In early childhood, they are extremely active. They trap bacteria and viruses, process them, and help train your adaptive immune system — producing IgA antibodies, coordinating B and T cell responses, and essentially functioning as a training ground for your developing immune architecture.
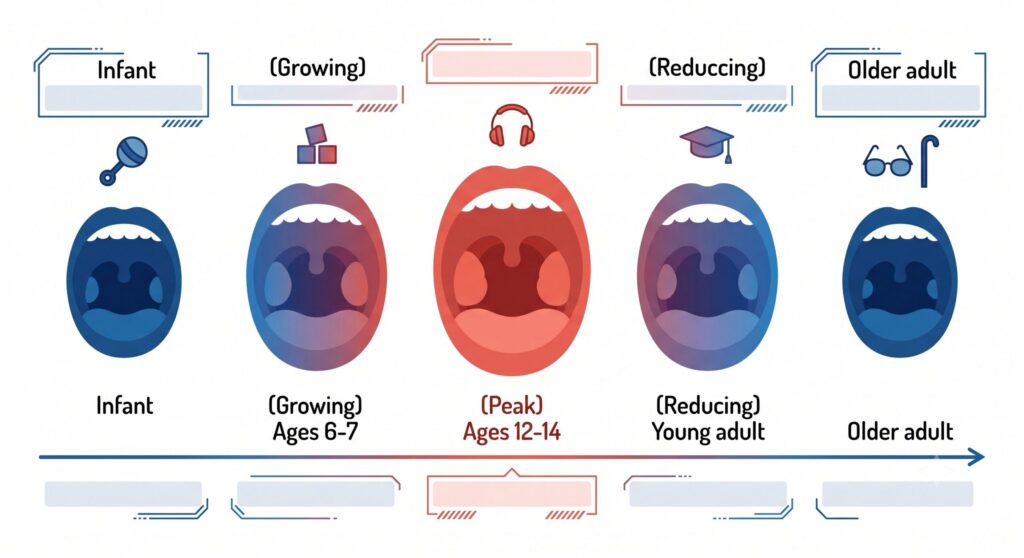
This is why tonsils are big in children. It is normal. From birth to roughly age six or seven, they grow rapidly as immune stimulation increases. Around ages twelve to fourteen, they reach their absolute peak size. Then, as the immune system matures and begins relying less on these mucosal sentinels, the tonsils start to involute — that is, undergo a process of gradual regression. Androgens released during puberty promote lymphoid tissue regression and fibrous replacement. Published longitudinal data from Japan tracking adenoid and tonsil sizes from ages six to twenty showed this arc clearly: approximately 200% growth by late childhood, followed by involution during adulthood. By old age, only a small remnant of tonsillar tissue typically remains.
So yes — tonsillar regression is real. In children and adolescents, it is the expected biological outcome. This is also why the natural history of recurrent tonsillitis in children often improves as they age into their late teens, even without surgical intervention.
The Problem: What Happens When Chronicity Sets In
Here is where the story gets more complicated. And this is the part that the social media posts about “tonsil regression” almost always miss.
The biology described above — healthy involution driven by immune maturation — applies to tonsils that are functioning normally, even if they are temporarily enlarged due to acute infection. It does not apply to tonsils that have crossed into chronicity.
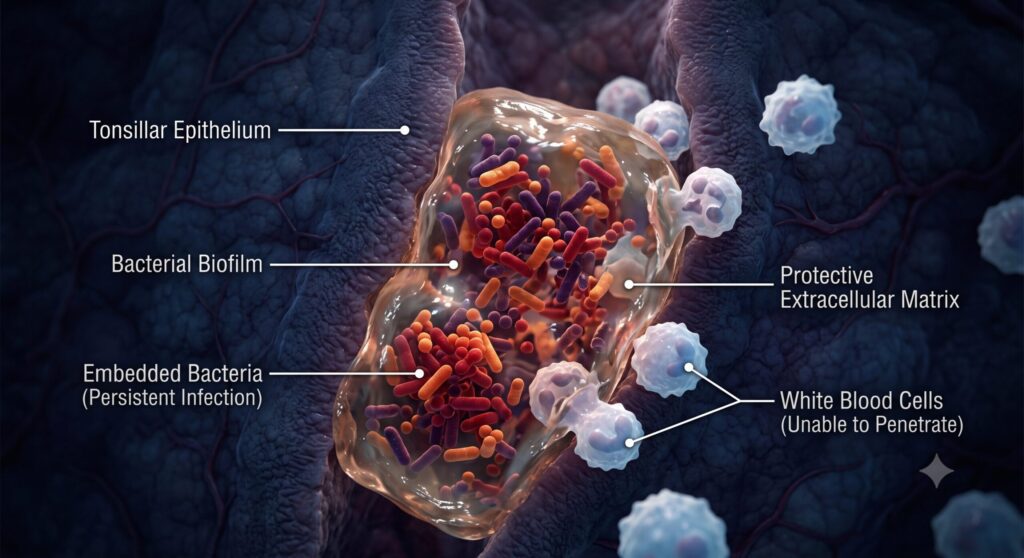
Chronic tonsillitis is a different beast from recurrent acute tonsillitis, and the distinction matters. In chronic tonsillitis, the tissue is no longer occasionally infected and then recovering. Instead, the tonsils have become persistently colonised, repeatedly inflamed, and structurally altered. The architecture of the tonsillar crypts — the deep channels that run through the tissue — becomes compromised. This is where biofilm comes in.
Bacterial biofilms are organised communities of bacteria that secrete a protective extracellular matrix around themselves. Inside this matrix, bacteria are shielded from both the immune system and antibiotics. Research published in 2025 in Biomedical Reports confirmed that biofilm formation is a key factor in the persistence and recurrence of tonsillitis specifically, and that biofilm-producing pathogens form protective matrices that actively resist immune defences and antimicrobial treatment.
Critically, a study examining 140 palatine tonsils from patients undergoing tonsillectomy at our centre found Staphylococcus aureus and Haemophilus influenzae as the predominant biofilm-forming organisms in chronic tonsillar disease. The biofilm mode of growth was directly associated with antibiotic treatment failure — organisms that appeared susceptible on standard laboratory testing were nonetheless surviving in the patient because the biofilm environment creates conditions that standard antibiotic concentrations cannot penetrate effectively.
This is not a treatment failure in the conventional sense. The antibiotic is not the wrong drug. The delivery mechanism is the problem. In biofilm, bacteria can tolerate concentrations of antibiotics many times higher than their minimum inhibitory concentration measured in standard in vitro testing. Each course of antibiotics clears the planktonic (free-floating) bacteria, which is why symptoms temporarily improve. But the biofilm community embedded in the tonsillar crypts survives, reseeds the tissue, and the cycle restarts.
So Can Medication Actually Shrink Tonsils?
This requires separating two things that patients — and occasionally, their doctors — conflate: reduction in tonsil size due to treating acute inflammation, versus genuine tissue regression in chronically diseased tonsils.
Corticosteroids can reduce tonsillar swelling meaningfully when the enlargement is driven by acute or subacute inflammation. A short course of steroids for a severe acute tonsillitis can visibly reduce tonsil size within days. But this is inflammatory oedema resolving, not glandular regression. When the steroids stop and re-exposure to pathogens occurs, the tissue responds as before.
Antibiotics suppress bacterial load and reduce acute symptoms. In mild or early disease, they may allow the immune system to regain enough control that the tonsils partially reduce in size over months. This is occasionally observed in children with first or second episodes of tonsillitis, where the disease has not yet progressed to biofilm-dominated chronicity. In adults with established chronic disease, this outcome becomes progressively less likely with each recurrence.
Anti-inflammatory medications (including long-term nasal steroid sprays sometimes prescribed off-label for lymphoid hypertrophy) have some evidence in adenoid reduction, particularly in children with obstructive adenoid hypertrophy. Their effect on established chronic tonsillitis in adults is limited.
Watchful waiting — doing nothing and simply observing — is appropriate, and indeed recommended, for patients who do not yet meet surgical thresholds. The Paradise criteria, the most commonly used clinical framework for tonsillectomy decisions, specifies that children not meeting the frequency and severity thresholds should be observed rather than immediately operated on. This reflects the biological reality that in younger patients especially, spontaneous improvement does occur. But watchful waiting is a structured clinical decision, not a passive alternative to treatment.
What medication cannot do, once true chronic tonsillitis with biofilm colonisation has established itself, is cure the underlying disease. It can manage symptoms. It cannot remove the structurally compromised tissue that has become a reservoir for recurrent infection.
Why “It Will Get Better on Its Own” Fails Adults With Chronic Disease
The involution narrative — that tonsils shrink as you get older — creates a particular problem for adult patients with recurrent tonsillitis. The logic goes: “I had bad tonsils as a child, but they got better as I grew up, so maybe this will too.” That experience was real. But by adulthood, the biological window for spontaneous lymphoid involution has largely closed.
A 2023 Lancet commentary on tonsillectomy in adults noted that the Paradise criteria were originally derived from paediatric clinical trials and were later extrapolated to adult guidelines without justifying research in adult populations. The implication is important: the evidence that watchful waiting leads to natural resolution is far stronger in children than in adults. In adults with documented recurrent acute tonsillitis — specifically those experiencing three to five episodes per year — the NATTINA trial (National Trial of Tonsillectomy in Adults) demonstrated that tonsillectomy produced significantly fewer sore throat days and improved quality of life compared to conservative management.
Adults with established chronic tonsillitis are not going to grow out of it. The trajectory, if left untreated, is continued recurrence, progressive antibiotic resistance due to repeated courses, and in some cases complications including peritonsillar abscess.
The Chronicity Threshold: When the Biology Changes
In clinical practice, the conversation about surgery typically becomes serious when:
Frequency crosses a threshold. Broadly accepted frameworks suggest seven or more documented episodes in one year, five or more per year for two consecutive years, or three or more per year for three consecutive years. The American Academy of Otolaryngology — Head and Neck Surgery recommends considering tonsillectomy after three or more infections per year despite adequate medical therapy. Each documented episode should involve a sore throat plus at least one of: fever above 38.3°C, cervical lymphadenopathy, tonsillar exudate, or a positive rapid strep test.
Antibiotics repeatedly fail or are repeatedly needed. If a patient requires four or five antibiotic courses in a year just to function, the antibiotic is functioning as a crutch rather than a cure. This is also the clinical scenario where antimicrobial resistance risk becomes a genuine concern at the individual patient level.
Complications develop. A peritonsillar abscess — a collection of pus that forms in the tissue surrounding a tonsil — occurring once raises the surgical threshold significantly. A second abscess is generally considered a firm indication for tonsillectomy in most guidelines, because the abscess represents a breakdown in the tissue’s ability to contain infection.
Obstructive symptoms emerge. When tonsil size causes airway obstruction during sleep — contributing to snoring, witnessed apneas, or frank obstructive sleep apnoea — the calculus changes. This is no longer an infection management question. It is an airway problem, and medication does not reliably reduce tonsil size enough to meaningfully address airway compromise in adults with significant hypertrophy. Polysomnography should be considered in patients with obstructive symptoms before definitive surgical planning.
Systemic complications are present. Chronic tonsillitis can act as a focal infection — driving systemic inflammation even when local signs are subtle. A 2025 case report from PMC documented a patient whose severe, unexplained systemic inflammatory symptoms resolved completely after tonsillectomy, with a decade of diagnostic workup having failed to identify the tonsils as the source. This is not common, but it is not vanishingly rare either, particularly when conventional biomarkers are normal and local signs are missed because tonsillar compression during examination was not performed.
Why Surgery Is Sometimes the Only Rational Choice
I want to be careful here. Tonsillectomy is not a minor procedure. It carries a small but real risk of post-operative bleeding — the most feared complication — occurring in roughly 1 to 3% of patients, with a small subset requiring return to theatre. Post-operative pain is significant, particularly in adults, and the recovery period is longer than most patients expect. These risks mean the decision to operate should always involve genuine shared decision-making between the surgeon and the patient.
But there is a version of “watchful waiting” that crosses from appropriate observation into avoidance, and that is worth naming directly. When a patient has had repeated antibiotic courses over two or more years, when the episodes are documented and frequent, when quality of life is substantially affected — the evidence supports surgery more strongly than continued conservative management.
The biological reality of established chronic tonsillitis is that the diseased tissue is not going to spontaneously normalise. The crypts that harbour biofilm are structurally part of the tonsil. You cannot debride them with medication. The inflammatory cycles that perpetuate the disease are driven by tissue that has been irreversibly altered. Short of removing it, there is no current medical therapy that reliably resolves this state.
A 2024 systematic review on treatment of recurrent acute tonsillitis published in European Archives of Otorhinolaryngology reached a practical conclusion that mirrors clinical experience: for patients with well-documented recurrent tonsillitis meeting frequency criteria, tonsillectomy remains the most effective intervention for reducing episodes and improving quality of life. The same review noted that even patients who did not strictly meet guideline thresholds reported significant quality of life improvements after surgery — suggesting that the current criteria, while useful, may undercount the functional burden of the disease.
One More Thing About Tonsil Size and OSA
Patients occasionally arrive at my sleep surgery clinic with moderate or severe OSA, and on examination the tonsils are contributing substantially to the airway obstruction — not through infection, but through sheer size. In these cases the question is not whether medication might regress the tonsils enough to solve the problem. The question is whether removing a large, obstructing, non-infected tonsil is the right surgical strategy as part of broader upper airway surgery.
For this group, the tonsillectomy decision sits within a different framework altogether. DISE — drug-induced sleep endoscopy — allows us to visualise the actual site and pattern of airway collapse during simulated sleep, and to determine how much the palatine tonsils are contributing relative to other collapsible structures. In tonsillar OSA, where the tonsils are grade 3 or 4 and the obstruction is predominantly at the oropharyngeal level, removing them can produce dramatic improvements in sleep-disordered breathing. Medication plays no role in this decision. The tissue is in the way.
The Bottom Line

Tonsils do shrink — spontaneously, as part of normal immune maturation during adolescence and early adulthood. This is real biology, and it is the reason watchful waiting is genuinely appropriate in many children and younger patients with early or mild disease.
What medication cannot do is reverse established chronic tonsillitis once biofilm colonisation has taken hold, or meaningfully reduce obstructive tonsillar hypertrophy in an adult whose airway is compromised. At that point, surgery is not aggressive or premature. It is the rational conclusion of a disease process that has outrun its medical alternatives.
If you have had repeated throat infections over the past year, or have been told your tonsils are enlarged and contributing to snoring or sleep problems, a proper clinical assessment — not a social media comment thread — is what will tell you where you actually sit in this spectrum.
Dr. Julius Goh Liang Chye is a Consultant Otorhinolaryngologist, Head & Neck and Sleep Surgeon at Universiti Malaya Specialist Center, Kuala Lumpur. To book for an appointment Click Here
FAQ SCHEMA
Q: Do tonsils shrink naturally as you get older? A: Yes — tonsillar involution is a normal biological process that begins around puberty and continues into adulthood, driven by immune maturation and hormonal changes. This is why recurrent tonsillitis often improves naturally in children and teenagers. However, in adults with established chronic tonsillitis, this window for spontaneous improvement has largely closed.
Q: Can medication shrink tonsils permanently? A: Medication can reduce tonsillar swelling caused by acute inflammation, and antibiotics can suppress bacterial infection temporarily. But in chronic tonsillitis where bacterial biofilm has colonised the tonsillar tissue, no current medication can reliably eliminate the disease or produce lasting reduction in tonsil size. Surgery removes the affected tissue entirely.
Q: Why do antibiotics keep failing for my recurrent tonsillitis? A: Repeated antibiotic treatment failure in chronic tonsillitis is usually related to bacterial biofilm. Bacteria living in biofilm within the tonsillar crypts are protected by an extracellular matrix that antibiotics cannot penetrate effectively, even when standard laboratory tests show the bacteria should be susceptible to the drug prescribed. Antibiotic courses clear the free-floating bacteria, which reduces symptoms temporarily, but the biofilm colony survives and reseeds the infection.
Q: When should I consider tonsillectomy? A: Broadly accepted clinical criteria suggest tonsillectomy should be considered for adults with seven or more documented tonsillitis episodes in a year, five or more per year for two consecutive years, or three or more per year for three consecutive years. Earlier surgery may also be indicated for peritonsillar abscess, antibiotic intolerance, or when enlarged tonsils are causing obstructive sleep apnoea. A proper ENT assessment is needed to determine which category applies to you.
Q: What happens if chronic tonsillitis is left untreated? A: Without treatment, chronic tonsillitis typically continues to recur. Each episode may require another antibiotic course, contributing to antimicrobial resistance at the individual level. Complications such as peritonsillar abscess can develop, which is a more serious and painful condition requiring surgical drainage. In some patients, untreated tonsillitis can act as a source of systemic inflammation affecting other organ systems.
Q: Is tonsillectomy safe for adults? A: Tonsillectomy is a common and well-established surgical procedure. Like all surgery it carries risks, the most important being post-operative bleeding in approximately 1–3% of patients. Recovery in adults typically takes 10–14 days and is more uncomfortable than in children. The decision should always involve a discussion of risks, benefits, and alternatives with your ENT surgeon.
References
- Empitu MA, et al. Pharmacological strategies for targeting biofilms in otorhinolaryngologic infections and overcoming antimicrobial resistance. Biomed Rep. 2025;22(6):95. https://pmc.ncbi.nlm.nih.gov/articles/PMC12001231/
- Abubakar S, et al. Evidence of bacterial biofilms among infected and hypertrophied tonsils in correlation with the microbiology, histopathology, and clinical symptoms of tonsillar diseases. ScientificWorldJournal. 2014. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3886491/
- Ogawa T, et al. Patterns of adenoid and tonsil growth in Japanese children and adolescents: a longitudinal study. Sci Rep. 2018;8:16974. https://www.nature.com/articles/s41598-018-35272-z
- Palacios-García I, et al. Role of germinal center and CD39highCD73+ B cells in the age-related tonsillar involution. Front Immunol. 2024. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11010345/
- Bauer M, et al. Chronic tonsillitis as a focal infection: a decade-long case involving severe systemic symptoms. PMC. 2025. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12875394/
- Bhutta MF. Tonsillectomy in adults — to do or not to do. Lancet. 2023;401(10385):1348–1349. https://www.thelancet.com/journals/lancet/article/PIIS0140-6736(23)00673-6/abstract
- Guntinas-Lichius O, et al. Treatment of recurrent acute tonsillitis — a systematic review and clinical practice recommendations. Eur Arch Otorhinolaryngol. 2024;281(1):1–20. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC10597714/
- Mehmood B, Bhimji SS. Tonsillitis. In: StatPearls [Internet]. Treasure Island (FL): StatPearls Publishing; 2025. https://www.ncbi.nlm.nih.gov/books/NBK544342/
- Bope ET, Kellerman RD. Peritonsillar abscess and cellulitis. In: Merck Manual Professional Edition. Updated May 2025. https://www.merckmanuals.com/professional/ear-nose-and-throat-disorders/oral-and-pharyngeal-disorders/peritonsillar-abscess-and-cellulitis
- Houborg HI, Klug TE. Evaluation of guidelines for tonsillectomy in adults with recurrent acute tonsillitis. Ann Otol Rhinol Laryngol. 2023;132(10):1197–1204. https://journals.sagepub.com/doi/10.1177/00034894231173481
Discover more from The ENT Doctor
Subscribe to get the latest posts sent to your email.
No responses yet