
Of all the consultations I find most thought-provoking, the ones involving a child with nasal problems sit near the top. The parent has usually done their research. They know their child is a mouth breather. They have noticed the blocked nose, the snoring, perhaps the slightly open-mouthed expression that never quite closes. A friend has suggested a deviated septum. Someone online said surgery fixed it in two weeks.
And then I have to explain that the nose their child has today is not the nose they will have in five years. That operating on a structure that is still reshaping itself carries risks that do not exist in adult surgery. And that the decision to wait is often the most technically sophisticated thing a surgeon can do.
But I also have to be honest about the other side: sometimes waiting causes real harm. Sometimes the nose is so severely blocked that the face itself is developing abnormally. In those situations, surgery is not optional — it is part of protecting the child’s development.
This post is my attempt to give parents the full picture.
The Growing Nose: Why Children Are Not Small Adults
The fundamental reason nasal surgery in children requires more caution than in adults is straightforward but frequently underestimated: the nose does not reach its final size and shape until mid-to-late adolescence, and some of its growth machinery lives inside the very structures a surgeon would be touching.
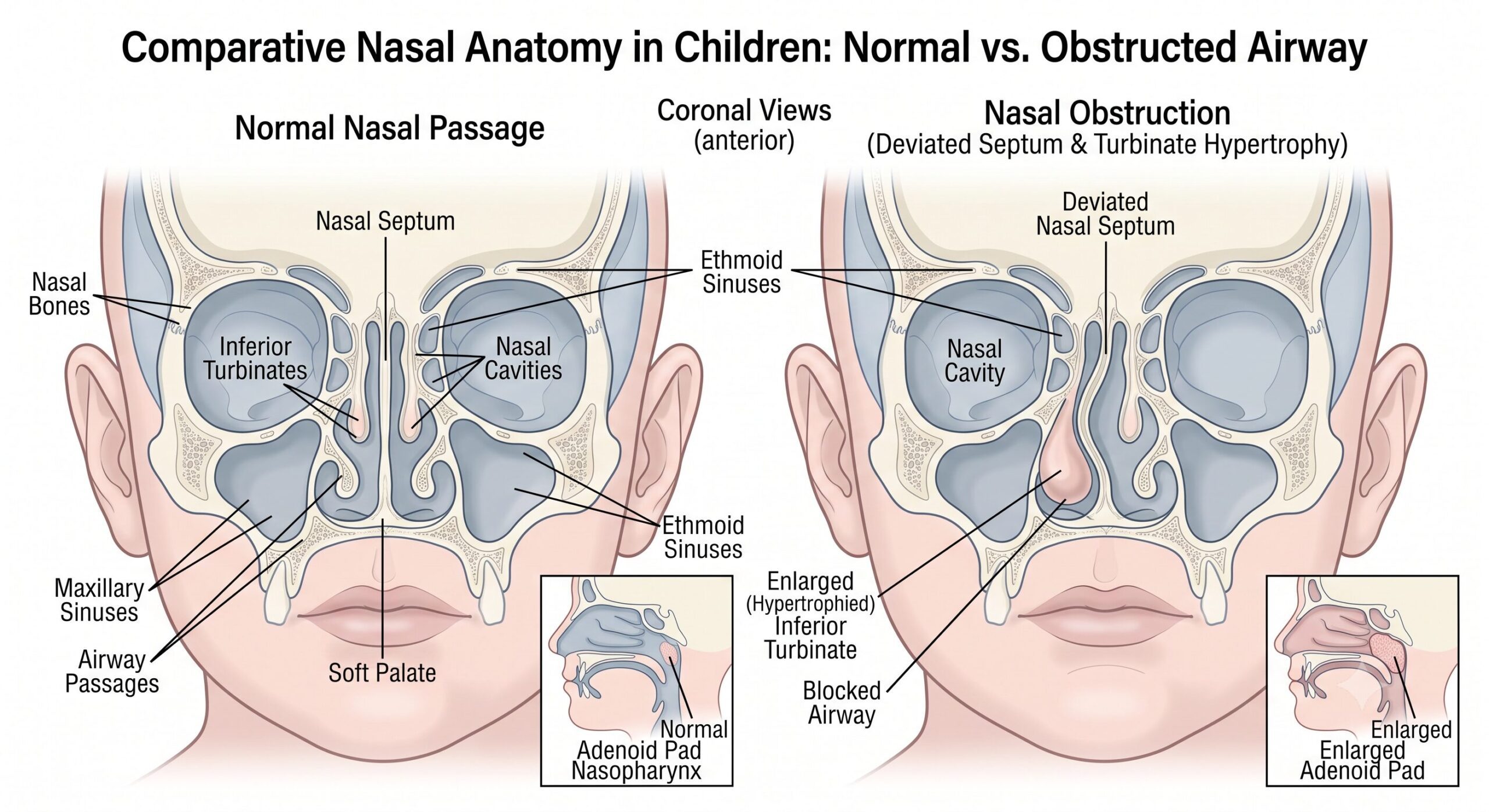
The nasal septum — the wall of cartilage and bone that divides the nose into two passages — is not merely a partition. It is an active growth centre. The cartilaginous septum pushes forward and downward as the face develops, driving elongation of the nose and contributing to outgrowth of the maxilla — the upper jaw. There are two specific zones within the septal cartilage, the sphenodorsal and sphenospinal zones, that are directly implicated in this process. When animal studies in the 1950s and 1960s removed large segments of septal cartilage without preserving the surrounding mucoperichondrium, the resulting animals showed stunted maxillary development and saddle nose deformities. Those early findings put nasal surgery in children firmly in the “wait” column for decades.
The consensus that emerged from subsequent research is that nasal and midface growth continues until approximately age 14 to 17 years. More precise estimates put it at 16 years for boys and 14 for girls, based on when the nose reaches 98% of its mature dimensions. The nasal septum itself continues to grow — more slowly — until around age 36. These numbers are not absolute cut-offs, but they give the clinical framework within which surgeons make decisions.
This is the biological reality parents need to understand: when a surgeon declines to operate on a ten-year-old’s deviated septum, they are not being overly cautious. They are protecting growth architecture that cannot be replaced once disrupted.
What the Evidence Actually Shows About Operating Early
The picture has become more nuanced over the past decade, and it is worth being direct about what the research does and does not say.
The 2025 Stanford meta-analysis — the largest systematic review to date on paediatric nasal surgery, covering 27,840 patients across 23 studies — found that septoplasty had the highest average age at surgery and the lowest complication and revision rates. Septorhinoplasty, by contrast, had the youngest average age at surgery and the highest complication and revision rates. The hierarchy is meaningful: the more extensively you operate on a child’s nose, the greater the likelihood you will need to do it again.
The revision rate difference is particularly telling. A major paediatric outcomes study found that children under 14 who underwent septoplasty had a revision rate of 14%, compared to 4.2% in those aged 14 and older. That is a three-fold difference. The younger the child, the higher the chance that growth will displace whatever was corrected.
A 2026 Springer review on paediatric septorhinoplasty confirmed that recent studies show septoplasty does not significantly affect midfacial growth, but revision rates are higher in children compared to adults undergoing nasal surgery. In other words: you can probably operate without stunting the face, but you are significantly more likely to need to come back and do it again.
For parents, this translates into a practical reality: early surgery often means two surgeries. And each additional operation carries its own risks, anaesthetic exposure, recovery burden, and scarring potential. That is a meaningful cost.
The Consequences of Not Operating — and Why This Changes the Calculation
Here is where the debate becomes genuinely difficult, and where I think the “wait” default needs to be interrogated rather than simply assumed.
Chronic nasal obstruction in children is not just inconvenient. It forces the child to breathe through the mouth, and mouth breathing, sustained over years of facial development, has documented structural consequences.
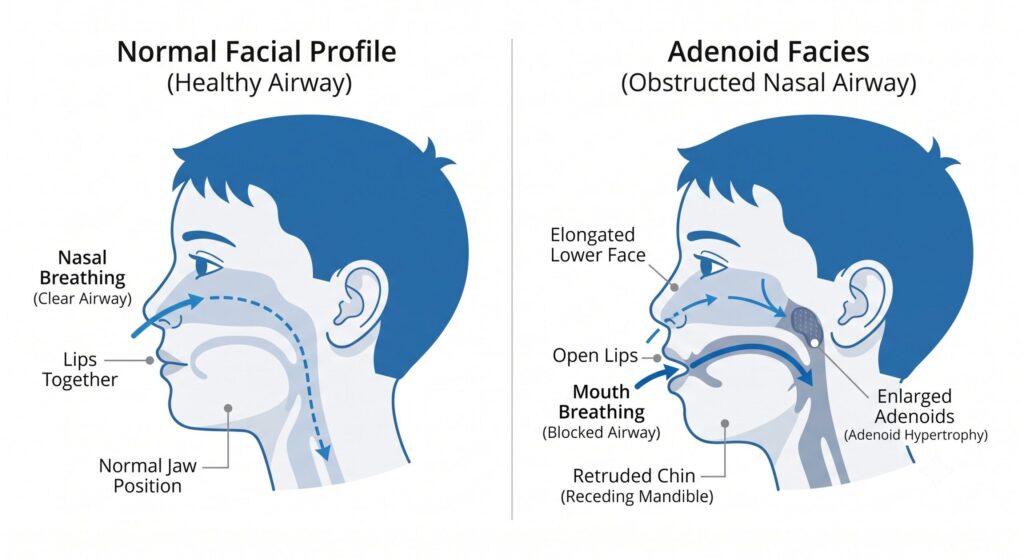
A 2025 umbrella review on mouth breathing and OSA in children found that chronic mouth breathing, often a compensatory adaptation to nasal obstruction, disrupts the functional equilibrium of the stomatognathic system. The absence of physiological nasal airflow and the abnormally low posture of the tongue alter the forces that shape the growth and development of maxillomandibular structures.The result is the clinical picture known as adenoid facies — a long, narrow face, high-arched palate, mandibular retrognathia, and increased anterior lower facial height. This is not a cosmetic concern. It is a structural deformation of the facial skeleton driven by abnormal breathing mechanics, and it happens precisely because surgery was delayed while the face was still growing.
A 2025 Frontiers in Allergy review noted that chronic nasal obstruction and resultant nocturtal mouth breathing are major causes or important aggravating factors for the development and progression of paediatric obstructive sleep apnoea, which disrupts sleep architecture, reduces deep sleep and REM sleep, and in severe cases may impact normal growth and development.
So the surgeon faces a genuine dilemma: operating too early risks disrupting the growth centres of the nose, but waiting too long allows the obstruction to deform the face and impair sleep. Neither outcome is acceptable. The skill lies in judging where a particular child sits on that spectrum.
Medical Management First — Always

Before surgery is considered for any child with nasal obstruction, a structured trial of medical management should be exhausted. This is not a formality. In many children, particularly those whose obstruction is driven by allergic rhinitis or adenoid hypertrophy rather than a fixed structural deformity, medical treatment resolves the problem entirely.
For allergic rhinitis with turbinate swelling, the first-line approach is intranasal corticosteroid sprays — fluticasone, mometasone, or budesonide — used consistently for eight to twelve weeks. Antihistamines and leukotriene receptor antagonists add benefit in children with concurrent allergy. These medications reduce turbinate size, improve nasal airflow, and in younger children with a still-reactive nasal lining, can produce substantial and durable improvement without any surgical intervention.
Saline irrigation — simple, safe, and cheap — reduces nasal mucosal oedema and clears allergens and mucus from the nasal cavity. Used twice daily, it is an underrated tool in the paediatric nasal obstruction toolkit.
Adenoid hypertrophy, which is the most common cause of nasal obstruction in children under ten, has its own surgical pathway that does not require touching the nasal septum or turbinates at all. Adenoidectomy — removing the adenoid pad from the back of the nasal cavity — is a well-established, relatively low-risk procedure with decades of evidence behind it, and it frequently resolves the obstruction without any need for septal or turbinate surgery.
A 2025 study in the International Journal of Paediatric Otorhinolaryngology confirmed that inferior turbinate reduction surgery is used in paediatric patients with turbinate hypertrophy who have failed medical management — the operative word being “failed.” Medical management is always the starting point.
When Surgery Becomes Unavoidable in Children
With all the above caveats firmly in place, there are circumstances where the clinical case for operating on a child’s nose — sometimes well before the conventional age thresholds — is compelling.
Severe structural obstruction causing airway compromise. A profoundly deviated septum that blocks one nasal passage near completely is not a candidate for nasal spray therapy. If the child cannot breathe through one side of their nose at all, and this is confirmed on endoscopy and objective nasal airflow measurement, the question of facial growth risk has to be weighed against the ongoing airway compromise. In these cases, a conservative septoplasty — preserving as much cartilage and mucoperichondrium as possible, correcting only what is functionally necessary — is justifiable at an earlier age than would otherwise be considered.
Post-traumatic nasal deformity. Nasal trauma in children, particularly from sports injuries or falls, can displace the septum in ways that cause immediate and severe obstruction. Facial Plastic Surgery Clinics guidance notes that in cases of trauma, corrective surgery should be carried out in a short time frame before scar contracture, aberrant remodelling, and malunion of structures occurs. The biological window for correcting a recent nasal fracture is short — typically within two weeks of injury before the bone sets. Missing this window means waiting considerably longer and dealing with a more complex correction later.
Congenital deformities. Conditions present from birth — choanal atresia, congenital midline nasal masses, significant cleft lip and nasal deformities — have their own surgical timelines that bear no resemblance to the “wait until sixteen” framework applied to routine septal deviations. Bilateral choanal atresia, in which both posterior nasal passages are blocked from birth, is a neonatal emergency — these infants are obligate nasal breathers who will die if the obstruction is not corrected immediately. A 2025 review on congenital nasal deformities noted that while surgical correction has historically been deferred until adolescence due to concerns about disrupting facial growth, emerging evidence supports earlier intervention, prompting a reevaluation of traditional paradigms.
Persistent OSA after adenotonsillectomy. Adenotonsillectomy is the first-line surgical treatment for paediatric OSA. But it does not always resolve the problem. StatPearls (updated December 2025) notes that persistent OSA following adenotonsillectomy may result from hypertrophy of the nasal turbinates, deviated nasal septum, adenoidal regrowth, lingual tonsil hypertrophy, or enlargement of the tongue base, and targeted surgical interventions addressing these specific anatomic abnormalities are required. When a child has been through adenotonsillectomy, still has documented OSA on polysomnography, and the residual obstruction is clearly nasal in origin — confirmed on endoscopy — nasal surgery moves from optional to necessary. Leaving a child with untreated OSA has well-documented consequences for neurocognitive development, behaviour, and growth.
Turbinate hypertrophy causing ADHD-like symptoms. This is an area where evidence has developed significantly in the past two years, and it deserves attention from parents whose children have been labelled as having attention difficulties. A 2025 retrospective cohort study found that inferior turbinate hypertrophy remains underrecognised in children with sleep-disordered breathing, and that inferior turbinate reduction was hypothesised to improve airflow, diminish sleep-fragmentation-driven SDB, and in turn attenuate ADHD-type behaviours. The inferior turbinates account for up to 50% of total nasal airway resistance. A child who cannot breathe through their nose at night, who sleeps poorly, who is irritable and inattentive during the day, and who has been put on ADHD medication without any assessment of their nasal airway — that child’s story may not have been correctly told yet. This is not to say all ADHD is nasal in origin. It is to say that nasal obstruction is worth ruling out before attributing behaviour problems to central causes.
What a Conservative Paediatric Nasal Operation Actually Looks Like
When surgery is warranted in a child, the approach should be deliberately more conservative than in an adult. The surgical objective is to relieve the obstruction — not to produce the perfect nose. Perfection can be pursued, if needed, once growth is complete.
For septoplasty in a child, this means conservative cartilage scoring or minimal resection rather than wide excision. The mucoperichondrium — the fibrous lining of the septum — must be meticulously preserved because it contains the cells responsible for cartilage healing and maintenance. Reimplantation of resected cartilage after remodelling, rather than discarding it, reduces the risk of saddle nose deformity. Growth centres, particularly at the osseocartilaginous junction and the dorsal and caudal struts of the septum, must be respected.
For turbinate reduction in a child, less invasive techniques — submucosal diathermy, radiofrequency ablation, coblation — are preferred over turbinectomy. The 2024 YO-IFOS consensus statement on paediatric inferior turbinate hypertrophy recommended that treatment choice should consider specific indications and features of available options, with a preference for less invasive procedures.The goal is to reduce the size of the turbinate while preserving its mucosal function — not to eliminate it. An empty nose in a child is a different and more complex problem than the one you started with.
A Word to Parents in the Consultation Room

The parent sitting across from me with a child who snores, breathes through their mouth, and has a nose that looks crooked on the outside deserves a complete explanation, not a reflexive “come back at sixteen.”
The question is always specific: what is causing this child’s obstruction, how severe is it, what are the measurable consequences, and how do the risks of operating compare to the risks of waiting? That calculation is different for a seven-year-old with mild turbinate swelling and controlled allergic rhinitis than it is for a twelve-year-old with a complete unilateral nasal blockage and documented sleep apnoea on overnight study.
What I tell parents is this: the nose is forgiving in children when you treat it with enough respect. But the developing face is not forgiving of a blocked airway left unaddressed for years. Get the assessment done properly — endoscopy, allergy testing, objective airflow measurement if indicated, sleep study if OSA is suspected — before anyone talks to you about an operating theatre.
If surgery does become the right answer, it should be done by a surgeon who has thought carefully about what to preserve, not just what to correct.
Dr. Julius Goh is a Consultant Otorhinolaryngologist, Head & Neck and Sleep Surgeon at Universiti Malaya Specialist Center, Kuala Lumpur. He is Chairperson of the Sleep Surgery Special Interest Group under CORLAMM (Academy of Medicine Malaysia) and a member of the International Sleep Surgery Society.
Kindly Click here for appointments
FAQ SCHEMA
Q: At what age can a child have nasal surgery? A: There is no single universal age. As a general guide, nasal growth is largely complete by around age 14 in girls and 16 in boys, and most elective nasal surgery is deferred until then. However, children with severe structural obstruction, post-traumatic deformity, congenital nasal conditions, or persistent sleep apnoea after adenotonsillectomy may require surgery earlier. The decision must be made individually after proper assessment.
Q: Can a child’s deviated septum be treated without surgery? A: In most children, especially younger ones, nasal obstruction from a deviated septum combined with turbinate swelling can be partially or substantially managed with intranasal steroid sprays, antihistamines, saline irrigation, and allergy treatment. Surgery is typically considered only after these measures have been tried and found insufficient. A proper ENT assessment including nasal endoscopy is needed to determine what is actually causing the obstruction.
Q: Does nasal surgery stunt facial growth in children? A: Extensive surgery — particularly submucous resection that removes large amounts of septal cartilage — can disrupt facial growth. Conservative septoplasty that preserves the mucoperichondrium and avoids key growth centres has been shown in multiple studies not to significantly affect midfacial development. The risk is primarily associated with how much cartilage is removed and how the surgery is performed, rather than with operating per se.
Q: What is adenoid facies and can it be prevented? A: Adenoid facies refers to the characteristic facial appearance that develops in children with long-standing nasal obstruction — typically a long, narrow face, open mouth, high-arched palate, and retruded lower jaw. It develops because mouth breathing alters the mechanical forces that shape the growing face. It can be prevented or limited by treating the nasal obstruction early enough — whether through medication, adenoidectomy, or in selected cases nasal surgery — before the facial skeleton has set.
Q: My child was diagnosed with ADHD but also snores — is there a connection? A: Possibly. Nasal obstruction that causes poor sleep can produce daytime inattention, hyperactivity, and irritability that closely resembles ADHD. Before attributing behavioural symptoms solely to a central cause, it is worth having the child’s nasal airway and sleep quality properly assessed. A sleep study and nasal endoscopy can determine whether obstructed nasal breathing is contributing to the sleep disruption driving the behaviour.
Q: When is nasal surgery genuinely urgent in a child? A: Bilateral choanal atresia in a newborn is a neonatal emergency requiring immediate surgical correction. Post-traumatic nasal deformity should ideally be corrected within two weeks of injury before malunion occurs. Persistent severe OSA after adenotonsillectomy, confirmed on polysomnography, that is driven by residual nasal obstruction also warrants prompt surgical planning. Outside these situations, most nasal surgery in children can and should wait for proper medical management to be attempted first.
References
- Patel RK, Loan P, Cendejas G, et al. Assessing the safety and efficacy of pediatric nasal surgery: a systematic review and meta-analysis. Facial Plast Surg. 2025. Epub Aug 5. https://pubmed.ncbi.nlm.nih.gov/40763773/
- Patel K. Congenital nasal deformities: advances in early surgical intervention. Plast Aesthet Res. 2025;12:70. https://www.oaepublish.com/articles/2347-9264.2025.70
- Springer Nature Link. Pediatric septorhinoplasty: why, how and when? Curr Otorhinolaryngol Rep. 2026. https://link.springer.com/article/10.1007/s40136-025-00536-6
- Bishop R, Sethia R, Allen D, Elmaraghy CA. Pediatric nasal septoplasty outcomes. Transl Pediatr.2021;10(11):2883–2887. https://pmc.ncbi.nlm.nih.gov/articles/PMC8649597/
- Fedok FG. Corrective nasal surgery in the younger patient. JAMA Facial Plast Surg. 2014;16(3):176–182. https://www.liebertpub.com/abs/doi/10.1001/jamafacial.2013.2302
- Nasal surgery in the younger patient. Facial Plast Surg Clin North Am. 2024. https://www.facialplastic.theclinics.com/article/S1064-7406(24)00061-0/pdf
- Ayad T, et al. Mouth breathing and obstructive sleep apnea in children: an umbrella review. J Clin Med.2025;14(2):13. https://www.mdpi.com/2694-2526/51/2/13
- Li X, et al. Clinical features, pathophysiological mechanisms, and multidisciplinary management strategies for rhinitis-induced adenoid facies in children and adolescents: a review. Front Allergy. 2025;6:1650119. https://pmc.ncbi.nlm.nih.gov/articles/PMC12436496/
- Ali AH, Digoy GP. Exploring the role of turbinate reduction in alleviating ADHD symptoms in pediatric patients. Cureus. 2025;17(7):e88807. https://pmc.ncbi.nlm.nih.gov/articles/PMC12377240/
- Maniaci A, et al. Pediatric inferior turbinate hypertrophy: diagnosis and management. A YO-IFOS consensus statement. Laryngoscope. 2024;134(3):1437–1444. https://pubmed.ncbi.nlm.nih.gov/37497872/
- Lee J, McColl LF, Meeker MO, et al. Evaluating utility of allergy testing in management of nasal obstruction following inferior turbinate reduction. Int J Pediatr Otorhinolaryngol. 2025;188:112177. https://www.sciencedirect.com/science/article/abs/pii/S0165587624003318
- Donnelly LF, et al. Pediatric obstructive sleep apnea. StatPearls [Internet]. Updated December 2025. https://www.ncbi.nlm.nih.gov/books/NBK557610/
Discover more from The ENT Doctor
Subscribe to get the latest posts sent to your email.
No responses yet