
Tonsil Stones: What TikTok Won’t Tell You
If you’ve spent any time on TikTok recently, you’ve probably stumbled across a tonsil stone video. Maybe it was a teenager squeezing a white lump out of her throat with a cotton swab. Maybe it was a doctor flushing out a crypt with a syringe. Either way, you probably couldn’t look away — and you probably spent the next ten minutes checking the back of your own throat in the bathroom mirror.
You are not alone.
The hashtag #tonsilstones has racked up billions of views. Tonsillectomy referrals in multiple published studies tracked upward in direct correlation with TikTok’s growth between 2016 and 2021. A published otolaryngology study described a doubling of tonsil stone clinic presentations — most of them anxious young women who’d watched a video and found nothing visibly wrong when an ENT actually examined them.
This is the other side of that viral content. So let’s talk about what tonsil stones actually are, why they keep coming back, what genuinely works, and — critically — when you need a surgeon versus when you just need a better toothbrush.
What Are Tonsil Stones, Really?
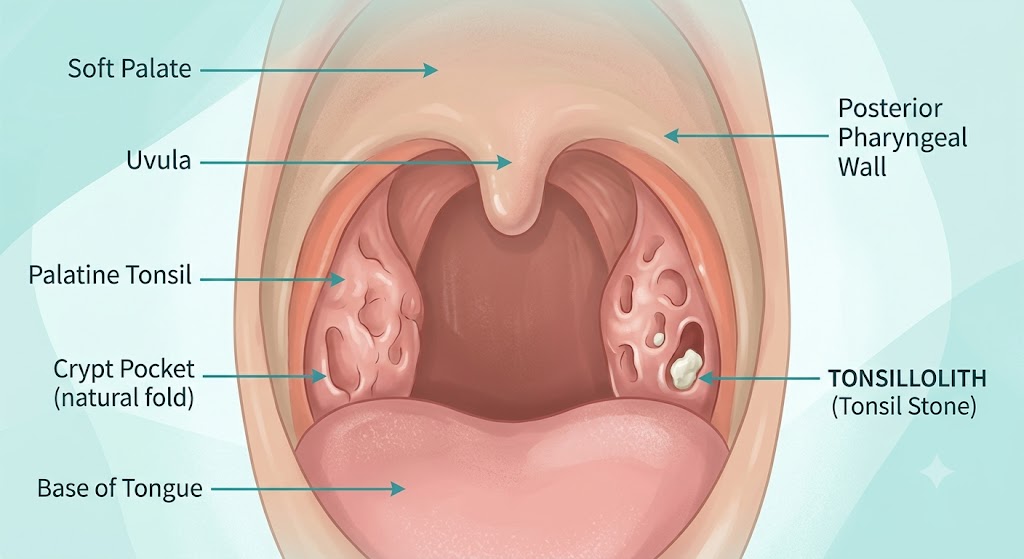
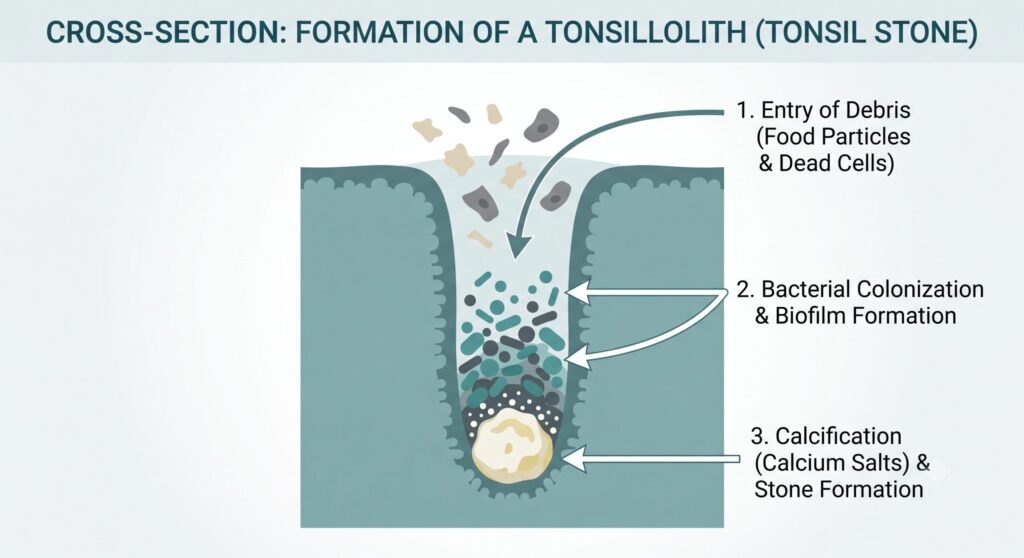
The medical term is tonsillolith (plural: tonsilloliths). They form in the small pockets and folds of the tonsils, called tonsillar crypts. These crypts trap dead cells, food debris, mucus, and bacteria. When that material builds up long enough, it calcifies — mostly through calcium salt deposition — and you get a hard, often white or yellowish lump that can range from a pinhead to, in unusual cases, the size of a marble.
They are not an infection in the conventional sense. But they are not just harmless debris either.
A key finding from research published in the journal Frontiers in Microbiology is that tonsil stones are actually a polymicrobial biofilm — a three-dimensional bacterial community held together by a protective matrix that the immune system cannot penetrate and antibiotics cannot adequately reach. The main bacterial species involved include Porphyromonas gingivalis and Fusobacterium nucleatum, both of which are also found in periodontal (gum) disease. A 2025 CBCT-based study in Scientific Reports found a notable overlap between the microbes in tonsilloliths and dental plaque biofilms — which means your gum health and your tonsil health are not as separate as you might think.
Risk factors for forming tonsil stones include:
- Chronically inflamed or scarred tonsils (from recurrent tonsillitis)
- Large tonsils with deep, prominent crypts
- Poor oral hygiene — especially inadequate tongue cleaning
- Dry mouth (reduced saliva means less natural self-cleansing)
- Post-nasal drip, which adds extra mucus to the crypt environment
- Smoking — promotes oral dryness and accelerates biofilm formation
The Most Common Symptoms (And One That Surprises People)
The classic complaint is bad breath that doesn’t go away even with regular brushing. That smell comes from volatile sulphur compounds produced by the anaerobic bacteria living inside the stone’s biofilm. If your breath has a persistent, somewhat rotten quality that doesn’t respond to mouthwash or mints, and your dentist has ruled out gum disease, tonsil stones are worth investigating.
Other symptoms include:
- A sensation of something stuck at the back of the throat
- Mild sore throat or throat discomfort that isn’t a full tonsillitis attack
- A white or yellowish visible lump on the tonsil surface
- Occasionally, referred earache (because the tonsil and ear share a nerve pathway)
- Difficulty swallowing, particularly with larger stones
Some tonsilloliths are found incidentally on dental X-rays, CT scans, or during a routine ENT check — patients had no idea they were there.
Why DIY Removal Keeps Failing
If you’ve watched those satisfying TikTok extractions and then tried it yourself, you’ve probably noticed that the stones come back. Sometimes within days.
That’s because DIY removal — cotton swab, water flosser pointed at the crypt, even the specialty tools sold online — addresses the stone but not the crypt. The anatomical pocket is still there. The biofilm environment is still there. The debris will accumulate again.
A few cautions worth stating clearly:
Don’t use sharp objects. The tonsil is highly vascular. The tonsillar pillars sit close to major vessels. Aggressive probing can cause significant bleeding.
Don’t let TikTok convince you that mucus gushing out equals “clearing your sinuses.” That particular myth applies more to the garlic-in-the-nose trend, but the same misunderstanding applies here — the body’s response to irritation is more mucus, not less.
Antibiotics will not clear tonsil stones. The calcified biofilm matrix physically blocks antibiotic penetration to the bacterial core. A course of amoxicillin may reduce surrounding inflammation during an active flare, but it will not dissolve the stone or prevent the next one.
The Treatment Ladder: From Conservative to Surgical
The right treatment depends on how frequently stones recur, how symptomatic they are, and whether concurrent tonsillitis is part of the picture.
Step 1 — Oral hygiene optimisation (all patients, always)
Start here. Genuinely. The tongue is the primary biofilm reservoir in the mouth. Most people brush their teeth reasonably well but never clean their tongue. Tongue scraping twice daily, thorough brushing of the back teeth and inner cheeks, and alcohol-free antimicrobial mouthwash (chlorhexidine gluconate works but shouldn’t be used indefinitely; cetylpyridinium chloride is a gentler long-term option) reduces the bacterial load available to seed crypt formation.
Saline tonsillar irrigation — using a curved-tip irrigator or water flosser on the lowest pressure setting directed carefully at visible crypts — is underused and genuinely helpful for maintenance. One case series reported no recurrence in a patient who maintained oral prophylaxis combined with bimonthly saline irrigation of the tonsillar site.
Step 2 — In-office manual removal
For single-episode management of a visible, accessible stone, gentle manual expression with a cotton swab or gloved finger is appropriate. Suction-assisted removal using an ENT suction tip is cleaner and better for multiple surface stones.
This is temporary by design. It manages the symptom without fixing the anatomy.
Step 3 — Tonsil cryptolysis (tonsil preservation surgery)
This is the step most people don’t know exists, and where the most interesting shift in management has happened over the past decade.
What is cryptolysis?
Instead of removing the tonsil, the surgeon obliterates the crypts — the pockets where stones form — by ablating (burning/vaporising) the crypt lining. The treated tissue scars and flattens, eliminating the space where debris can accumulate. The tonsil stays in place. Immune function is preserved.
CO₂ laser cryptolysis was the original technique. Precise, effective, and performed under local anaesthesia as an office procedure. Patients typically return to a normal diet within 24 hours. The main practical problem is that CO₂ laser equipment carries real risks — airway fire, retinal scatter, tissue plume — and the cost and safety requirements of running a medical laser suite make it inaccessible at most centres.
Coblation cryptolysis is now the preferred technique at most specialised ENT centres. Coblation uses low-temperature radiofrequency energy (40–70°C) — much cooler than conventional electrocautery — to ablate the crypt tissue with minimal collateral thermal damage. It was introduced as a laser alternative in a landmark 2012 case series by Chang and Thrasher published in the Ear, Nose & Throat Journal, and has since been validated in larger studies including a 2021 randomised controlled trial from Egypt’s Journal of Otolaryngology (n=105) that directly compared it head-to-head with cold dissection and monopolar/bipolar tonsillectomy.
The coblation arm showed significantly shorter operative time, less intraoperative bleeding, lower analgesic consumption, and faster return to normal diet — with equivalent or better symptom relief. No airway fire risk. No plume. No laser suite required.
Published follow-up data puts stone recurrence reduction above 80% at 12 months.
Who is a good candidate for cryptolysis?
- Recurrent, symptomatic tonsil stones
- No significant history of recurrent acute tonsillitis (≥4 documented episodes per year)
- Preference to preserve the tonsil
- Wanting to avoid the morbidity and haemorrhage risk of tonsillectomy
- Adults who cannot afford 10–14 days away from work
The procedure is performed under local anaesthesia. Most patients drive themselves home. Pain is manageable with simple analgesia for a few days.
Step 4 — Tonsillectomy (surgical removal of the tonsils)
Tonsillectomy is definitive. No tonsils, no crypts, no stones. Full stop.
But “definitive” does not mean “always the right choice.” In adults, tonsillectomy carries considerably more morbidity than in children, and this is something social media does not communicate honestly.
What to know before agreeing to a tonsillectomy for tonsil stones:
Post-tonsillectomy haemorrhage (PTH) is the key risk, and it is more common in adults than almost anyone expects. NHS hospital episode statistics for England (2016–2022), covering nearly 180,000 tonsillectomies, showed that adults required return to theatre for haemorrhage arrest at 3.5–3.8% — more than three times the rate in children (1.16%). Secondary haemorrhage typically peaks between day 5 and day 7 as post-operative scabs begin to separate.
Risk factors for bleeding include: male sex, current smoking, history of recurrent tonsillitis, and perioperative NSAID use. If you smoke, you need to stop well before any tonsil surgery — the risk increase is around 3.5-fold.
Recovery takes 10–14 days of significant pain and dietary restriction for most adults. This is not a comfortable recovery. Throat pain is often felt in the ears due to referred pain pathways. Eating and drinking early (even though it’s uncomfortable) actually helps healing and reduces complications — do not avoid it.
Tonsillectomy is appropriate when:
- Cryptolysis has failed, or the patient declines it
- Concurrent recurrent acute tonsillitis (≥4 episodes per year) is present
- A history of peritonsillar abscess (quinsy) exists
- A submucosal or deeply embedded stone requires open surgical access
- The patient fully understands the recovery and accepts the tradeoff
One important technical note: intracapsular tonsillectomy (tonsillotomy) — a partial removal that leaves the tonsil capsule — is increasingly used in children for obstructive sleep apnoea because it produces less pain and lower haemorrhage rates. For tonsil stones specifically, it is not the right choice. A published retrospective series found significantly higher stone recurrence at 6 months with the intracapsular approach, because residual crypt tissue can still harbour stone formation.
The TikTok-Driven Patient: What the Clinic Sees

Published ENT research has now documented what many Malaysian ENT specialists are observing in practice: a significant proportion of patients arriving requesting tonsillectomy for tonsil stones have no visible stones on examination, have not had recurrent tonsillitis, and are distressed adolescent females who traced their concern back to a social media video.
This is not a reason to dismiss the concern. Tonsilloliths are genuinely unpleasant. Bad breath and throat discomfort are real quality-of-life issues. But the answer for a teenager with borderline visible crypts and no documented infection history is not a tonsillectomy. It is an accurate diagnosis, reassurance, and structured oral hygiene guidance.
If you’re in that group — watching this content, wondering about your throat — book an ENT review before trying anything more invasive. The clinic visit will either find something worth treating or rule out something that was worrying you unnecessarily. Either outcome is better than ordering a stone removal kit from an online marketplace.
When Should You See an ENT?
See an ENT specialist for tonsil stones if:
- The bad breath or throat discomfort significantly affects your daily life or relationships
- Stones are recurring more than once a month
- You notice large, persistently uncomfortable stones that manual removal doesn’t resolve
- You have concurrent frequent throat infections
- You’ve tried improved oral hygiene for 4–6 weeks without improvement
- You want a proper diagnosis before deciding on any treatment
A good ENT assessment for tonsil stones will include a direct examination of the tonsils, possibly a nasoendoscopy if there’s any question about deeper pathology, and an honest conversation about whether observation, cryptolysis, or tonsillectomy makes sense for your particular anatomy and symptom burden.
A Note on Adenoliths
A 2009 paper in the International Journal of Pediatric Otorhinolaryngology coined the term “adenoliths” for stone-like calcified biofilm deposits found in the adenoid crypts — structurally and microbiologically similar to tonsilloliths. They’re worth knowing about because symptoms attributed to tonsil stones occasionally originate from the adenoid, particularly in patients with significant post-nasal drip and nasal obstruction. If your tonsils look clean but the symptoms persist, this is worth raising with your ENT.
Bottom Line

Tonsil stones are real, common, and genuinely disruptive. They form because of crypt anatomy combined with biofilm accumulation — not because of poor hygiene alone, and not because of anything that a cotton swab or a viral TikTok remedy will fix long-term.
The treatment that most patients don’t know about — coblation cryptolysis — preserves the tonsil, requires only local anaesthesia, sends you home the same day, and reduces recurrence by over 80% at 12 months. Tonsillectomy remains the definitive solution when the clinical picture warrants it, but in adults, the morbidity and haemorrhage risk deserve careful informed consent, not an impulsive booking after watching a satisfying extraction video.
If you’re based in Kuala Lumpur or Petaling Jaya and want a proper assessment, book a consultation at our ENT clinic. We’ll examine what’s actually there — and if treatment is needed, give you the full picture of your options before anyone picks up an instrument.
Links
TikTok Influence on Rates of Tonsillectomies for Tonsil Stones
Bleeding in Tonsillectomies
Tonsil Cryptolysis
Discover more from The ENT Doctor
Subscribe to get the latest posts sent to your email.
No responses yet