
You get a headache before the afternoon storm rolls in. Someone in your family office immediately says “sinus lah.” You take a Panadol, drink some warm water, maybe lie down under the ceiling fan. By evening it’s gone.
Most headaches end this way. Most. Not all.
What I want to do in this post is give you a practical framework for something that confuses almost everyone — and I mean everyone, not just patients. Even doctors get it wrong. The confusion is: when is a headache genuinely an ENT problem, when is it something else entirely, and most critically, when is it the kind of headache you should not be sleeping off at home?
Let’s go through it.
Why “sinus headache” is the most over-diagnosed condition in Malaysia
Here’s a statistic that still surprises me, and I work in this field: studies suggest that up to 95% of people who think they have a sinus headache actually have a migraine.
Not a little bit. Not half. Ninety-five percent.
The American Migraine Study II — one of the largest headache studies ever conducted — found that among nearly 30,000 participants, the most common misdiagnosis for migraine was sinus headache. A PMC review of 130 headache patients found that 81.5% had been incorrectly labelled as sinusitis before they got a proper diagnosis.
Why does this keep happening? Because the symptoms genuinely overlap.
Migraine activates the same nerves that supply your sinuses, eyes, ears, and jaw. When those nerves fire, you get facial pressure, nasal congestion, and watery eyes — symptoms that feel indistinguishable from a sinus infection to someone who’s never been formally evaluated. So the patient thinks “sinus.” The GP thinks “sinus.” Sometimes even the first ENT visit produces the same conclusion.
The result, in many cases, is years of unnecessary antibiotics, decongestants, even sinus surgeries that don’t help — because the sinuses were never the problem.
What a true ENT-related headache actually looks like

That said, headaches that genuinely originate from the nose, sinuses, and related structures are real — and I see them regularly. Here’s what distinguishes them.
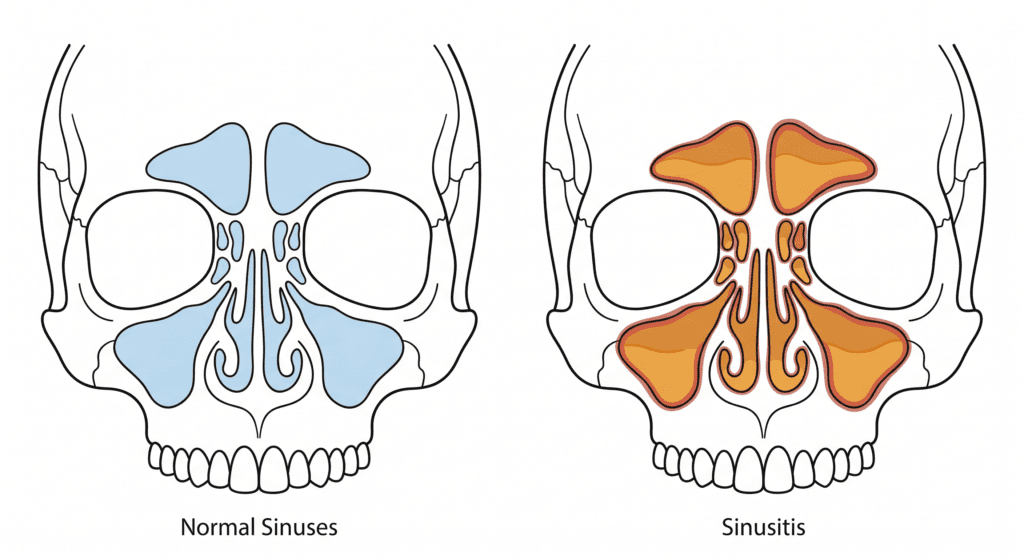
Acute sinusitis headache follows a recognisable pattern. There’s typically a preceding upper respiratory infection — a bad flu or cold — after which the nasal congestion doesn’t clear. Instead, facial pressure builds, usually over the cheeks or forehead, worsening when you bend forward. The nasal discharge is thick and discoloured (yellow or green, not clear). You may have a fever. There’s often a reduced sense of smell, and sometimes bad breath.
This is a real sinus headache. The sinuses are infected, inflamed, and blocking drainage. Treatment targets the infection. The headache goes when the infection resolves.
Chronic sinusitis headache is subtler. The pressure is duller, more persistent, sometimes described as a heaviness rather than sharp pain. It’s often worse in the morning and eases slightly as the day goes on. Nasal congestion is a constant companion rather than an acute feature. These patients often have anatomical factors contributing — a deviated septum, nasal polyps, or turbinate hypertrophy — and they’ve frequently been told they have “recurring sinus infections” for years.
Nasal and sinus headaches from structural issues can be triggered or worsened by specific things: stepping from cool aircon into hot humid air outside (a classic Malaysian trigger), haze season when particulate matter inflames the nasal lining, allergic rhinitis flares during specific seasons, or even swimming. The pressure is localised to the face rather than diffuse across the whole head.
The one feature that’s genuinely useful as a quick rule of thumb: if you have significant nasal symptoms — congestion, discharge, altered smell — alongside the head pain, there’s more reason to consider an ENT cause. If your nose is completely normal during the headache, it’s much less likely to be a sinus problem.
The Malaysia-specific triggers that genuinely do affect your sinuses
A few things deserve mention because they’re so common here that they get normalised.
The aircon-to-outdoors temperature swing. Kuala Lumpur exists in a state of constant micro-climate warfare. You step out of a 19°C office into 34°C humidity, then back into a 19°C car, then into a 22°C mall. This rapid cycling dries and then re-irritates the nasal mucosa, which in people with underlying rhinitis or structural issues can trigger genuine facial pressure and headache. It’s not imaginary. It’s also not really treatable by Panadol — it’s a nasal inflammation problem.
Haze. PM2.5 and PM10 particles from haze directly irritate the nasal lining and can trigger sinusitis in people who are already predisposed. During bad haze periods, we see spikes in ENT clinic attendance that track directly with API readings. If your headaches cluster around haze season and come with nasal symptoms, that’s meaningful information.
The before-the-rain phenomenon. This one is everywhere on TikTok right now, and it’s real. Changes in barometric pressure — the atmospheric weight that drops before a storm system moves in — create an imbalance between outside air and the air inside your sinuses. When that pressure can’t equalise quickly, people feel facial pressure, fullness in the ears, and head pain. But here’s the thing: this mechanism is also a known migraine trigger. So “I always get a headache before rain” does not by itself tell you whether you have a sinus problem or a migraine. Both can respond to barometric pressure change. You need the other accompanying symptoms to tell them apart.
What makes a headache NOT an ENT problem
Some headaches are not coming from your nose or sinuses at all, and treating them as if they are wastes time and risks real harm.
Migraine is the big one. The features that distinguish migraine from sinus headache: the pain is often one-sided and throbbing (though not always); nausea and vomiting are common; light sensitivity (photophobia) and sound sensitivity (phonophobia) are classic signs; the person wants to lie down in a dark, quiet room. The nasal discharge, if present, is usually clear and watery — not thick or discoloured. Migraines are not cured by antibiotics or nasal sprays, which is why patients who’ve been misdiagnosed spend years getting nowhere.
Tension headache is the most common headache type overall. It feels like a band of pressure around the head — both sides, usually. No nausea. No particular light sensitivity. No nasal symptoms. It’s dull, persistent, and typically comes from stress, poor sleep, or prolonged screen time. Very common among Malaysian office workers spending twelve hours staring at a screen under fluorescent lights in an over-airconditioned room.
Cluster headache is rarer but brutal — sudden, excruciating pain around one eye, occurring in clusters of attacks over weeks. The eye on the affected side often waters, the nostril may run. This can be confused with an ENT problem, but the pattern of attacks is distinctive. Anyone with this pattern should be properly evaluated.
Cervicogenic headache — originating from the neck — is another common miss. The pain starts at the back of the head and radiates forward. Prolonged use of a laptop on a low table, sleeping in a bad position, or hours on a phone with the neck bent down all create it. No amount of nasal treatment will help because the problem is musculoskeletal.
The red flags that mean you stop reading and go to A&E now

This is the section I want you to share with everyone you know.
Most headaches — even severe ones — are not dangerous. But some headaches are emergencies. And the difference is not always how bad the pain is. It’s about the pattern.
Thunderclap headache. A sudden, explosive pain that hits maximum intensity within seconds. Often described as “the worst headache of my life” — a phrase that should trigger immediate evaluation without exception. This can be a subarachnoid haemorrhage: bleeding around the brain from a ruptured aneurysm. It is fatal if missed and treated rapidly when caught. If you or someone near you experiences this, call an ambulance. Do not drive to clinic. Do not take Panadol and wait.
Headache with neck stiffness and fever. This combination — especially in a younger person — may indicate meningitis. An infection of the membranes around the brain. Also a medical emergency. If you can’t touch your chin to your chest, or someone near you suddenly develops a severe headache plus fever plus stiff neck, go to A&E immediately.
Headache with neurological symptoms. Weakness in the arm or leg, facial drooping, slurred speech, sudden vision changes, confusion, or difficulty walking alongside a headache means stroke or bleeding until proven otherwise. This is not a wait-and-see situation.
New headache in someone over 50 who doesn’t normally get headaches. A new pattern of headache after age 50 deserves investigation, not just pain relief.
Headache that wakes you from sleep or is consistently worst on waking. Most primary headaches — tension, migraine — are not typically present on waking. A headache that drags you out of sleep or greets you the moment you open your eyes can indicate raised intracranial pressure.
Headache that progressively worsens over days to weeks. A headache that keeps getting worse, rather than coming and going, needs imaging.
The mnemonic used in clinical medicine is SNOOP: Systemic symptoms (fever, weight loss), Neurological signs, Onset that is sudden, Older patient with new headache, Previous pattern change. Any of these present alongside a headache shortens the diagnostic process considerably — you’re moving toward imaging and specialist referral, not more decongestants.
So when should you actually see an ENT for your headaches?
The honest answer is: when the headaches are accompanied by clear nasal or sinus symptoms — congestion, discharge, altered smell, facial tenderness on pressing the cheeks or forehead — especially after a recent respiratory infection or during haze season.
An ENT assessment for headaches typically involves a detailed history, nasal endoscopy to directly visualise the nasal cavity and sinus openings, and sometimes a CT scan of the sinuses. This gives a definitive answer — either the sinuses show pathology that explains the symptoms, or they don’t, and you need to be referred to neurology for a primary headache evaluation.
What I’d rather not see is someone who’s been treating “sinus headaches” with repeated antibiotic courses for two years without anyone ever looking inside the nose with a scope.
If you’ve had recurring headaches for months and nobody has scoped your nasal passages yet, that’s a reasonable starting point.
The practical takeaway

Headache with nasal symptoms, facial pressure, coloured discharge, and a preceding infection: likely an ENT problem. See an ENT.
Headache with nausea, light sensitivity, one-sided throbbing, and normal nasal passages: likely migraine. See a GP or neurologist.
Headache with neck and shoulder tension, both-sided pressure, and a twelve-hour screen day behind you: likely tension headache. Take a break, fix your posture, sleep properly.
Headache that hits like a thunderclap, comes with a stiff neck and fever, or arrives alongside neurological symptoms: stop reading, go to A&E now.
Most headaches are benign, manageable, and figure-out-able with the right specialist. Some aren’t. Knowing which is which is genuinely worth knowing.
Dr. Julius Goh Liang Chye is a Consultant Otorhinolaryngologist, Head & Neck and Sleep Surgeon at Universiti Malaya Specialist Center (UMSC). For nasal, sinus, and ENT-related headache assessment, visit theentdr.com or contact us here
Further reading on theentdr.com:
- Why Malaysians keep getting sinus infections and why antibiotics keep failing them
- What haze season does to your nose, sinuses, and throat
- What aircon is doing to your nose every day
External Links
Discover more from The ENT Doctor
Subscribe to get the latest posts sent to your email.
No responses yet